
| From artists to athletes, these biopics portray bipolar disorder with empathy — without reducing anyone to a diagnosis. Sometimes, Hollywood gets it right. On-screen stories about the bipolar experience can help foster empathy and educate audiences. The following movies tell the narratives of real people with bipolar disorder, from famous writers and painters to athletes. Although the films delve into the symptoms of bipolar and the impact a brain-based disorder has on the lives and careers of the characters, their identities are never reduced to their diagnosis. Seeing your journey reflected in a story can be a powerful reminder that you’re never alone. Exploring the Life of Jackson Pollock in Pollock Starring Ed Harris and Marcia Gay Harden, this 2000 docudrama portrays Jackson Pollock’s life of art, struggle, and love. The abstract expressionist was famous for his distinctive drip painting style. Throughout his life, Pollock battled with alcoholism, and although the film does not explicitly name bipolar disorder, the connection to his mood cycles is implied. Pollock’s story illustrates the complex relationship between creativity and the management of a psychiatric condition. Cobb: A Complicated Look at Baseball’s Ty Cobb Al Stump is a celebrated sports journalist selected by baseball great Ty Cobb (played by Tommy Lee Jones) to author his official, authorized, and sugar-coated “autobiography.” To put it mildly, Cobb is a difficult figure, and he doesn’t want to leave this world without telling his side. Historical accounts report that he was prescribed lithium — a common mood stabilizer — during his last years. Click to Read More Melinda Source: https://www.bphope.com/bipolar-buzz/7-best-biographical-movies-featuring-bipolar-disorder/?utm_source=iContact&utm_medium=email&utm_campaign=bphope&utm_content=BUZZ+-+Mar1+-+Movies |
|---|
Category: Mental Illness
15 Elite Athletes Living With Bipolar Disorder, Depression, or Anxiety
From Olympic podiums to the Super Bowl, these athletes have used their platforms to show that mental health challenges can affect anyone.
Elite athletes endure relentless pressure to perform, often facing fierce public scrutiny in a culture that has historically discouraged seeking help. From an early age, these competitors are conditioned to be invincible — physically superior and mentally bulletproof. Yet, physical strength offers no immunity to clinical depression, anxiety, or bipolar disorder. Performance anxiety, the isolation of injury, and the weight of expectation can take a serious psychological toll.
Fortunately, the tide is turning. A growing number of sporting legends are shattering the silence, proving that mental well-being is just as critical as physical conditioning. By sharing their stories, these athletes are dismantling stigma and redefining what it means to be strong.
Tyson Fury (Boxing)
British heavyweight boxing champion Tyson Fury, known as “The Gypsy King,” has spoken publicly about living with bipolar disorder. Despite dethroning Wladimir Klitschko in 2015, Fury spiraled into a dark depression that included substance use and suicidal ideation, famously revealing that he nearly drove his Ferrari off a bridge during his lowest moment. Diagnosed with bipolar in 2017, he credits his recovery to his Christian faith, family, and a disciplined return to training. With a scheduled return to the ring on April 11, 2026, against Arslanbek Makhmudov, Fury continues to act as a powerful voice for destigmatizing mental illness. “I have flaws, and I have many of them,” he once said. “But I’m an ambassador for mental health.”
Terry Bradshaw (NFL)
While celebrated as a four-time Super Bowl champion and NFL Hall of Famer, Terry Bradshawis equally prolific as a broadcaster, actor, and musician. However, behind the public persona, he struggled silently until a diagnosis of clinical depression in 1999. Following years of anxiety attacks, intense anger, and alcohol abuse, Bradshaw found stability through medication, therapy, and faith. He remains unapologetic about his journey. “You know what, I’m not ashamed of who I am,” he told esperanza magazine. “It’s the way I was made. I just got some issues here, and I dealt with them. And I’m proud of it.”
Simone Biles (Gymnastics)
Widely considered the greatest gymnast of all time, Simone Biles changed the definition of strength when she withdrew from the Tokyo Olympics to protect her mind and body from “the twisties ” — a dangerous mental block. She prioritized her safety over gold medals, sparking a global conversation about the pressure placed on elite athletes. Biles returned to the world stage at the 2024 Paris Olympics with a renewed perspective, proving that taking a step back is often the bravest move of all. “I have to focus on my mental health and not jeopardize my health and well-being,” she said. “It’s okay not to be okay.”
Dwayne Johnson (WWE/Film)
Originally known as one of the greatest professional wrestlers of all time, Dwayne “The Rock” Johnson has successfully transitioned into a global superstar on the big screen. Recently, he drew attention for a dramatic turn in the A24 biopic The Smashing Machine (2025), portraying MMA legend Mark Kerr’s battle with addiction. Despite his massive success, Johnson has been remarkably open about his own history of major depressive disorder, using his platform to encourage men to seek support. He emphasizes that psychological well-being is as vital as physical strength. A dedicated father and philanthropist, Johnson actively contributes to social causes ranging from animal welfare to natural disaster relief.
Michael Phelps (Swimming)
As the most decorated Olympian in history, swimmer Michael Phelps has been candid about the price of perfection. He revealed to esperanza magazine that he spiraled into deep depression, anxiety, and substance use even while at the peak of his career. “With athletes or celebrities, people think they’re so much different than everybody else,” he said. “But I’ve gone through the same troubles.” In December 2025, Sports Illustrated honored Phelps with the Muhammad Ali Legacy Award for his enduring commitment to mental health advocacy.
A.J. Mendez (WWE)
Retired WWE superstar and author A.J. Mendez (formerly known as AJ Lee) is dedicated to combating the stigma surrounding bipolar disorder. Now a New York Times best-selling author and executive producer of WOW (Women of Wrestling), Mendez uses her platform to discuss her bipolar diagnosis. In her memoir, Crazy Is My Superpower, she detailed her childhood struggles and the cultural pressure to hide weakness, specifically challenging the “machismo” often found in the Puerto Rican community. Although she retired in 2015, Mendez made headlines with a surprise return to WWE SmackDown in late 2025.
Naomi Osaka (Tennis)
As a four-time Grand Slam champion, tennis superstar Naomi Osaka made headlines not just for her dominance on the court, but for her refusal to compromise her peace. In 2021, she withdrew from the French Open to prioritize her mental health, revealing a long battle with depression and anxiety that made mandatory press conferences unbearable. Her decision forced the sports world to re-evaluate how it treats athletes. After taking time away to become a mother, Osaka returned to tennis with a mission to advocate for player well-being. “I felt like it was important to stand up for myself,” she said. “And I hope that my actions encourage others to do the same.”
Kevin Love (NBA)
For years, NBA champion Kevin Love struggled in silence, viewing his challenges as a weakness he had to hide. That changed in 2017 when he experienced a panic attack during a game, leaving the court unable to catch his breath. He later penned a groundbreaking essay, “Everyone Is Going Through Something,” which dismantled the stigma of vulnerability in men’s sports. Love founded the Kevin Love Fund to provide mental health education and support. “Nothing haunts us like the things we don’t say,” he wrote. “So if you’re reading this and you’re having a hard time, you’re not alone.”
Chamique Holdsclaw (WNBA)
WNBA legend and Olympic gold medalist Chamique Holdsclaw was initially treated for major depression, but later re-diagnosed with bipolar disorder after antidepressants triggered a manic episode and impulsive spending sprees. She has since turned her struggles into advocacy. “I want others to understand it can get better. I went through a period when I had no hope, when I didn’t want to be here,” she revealed to bp Magazine. “I hope they see my journey and get inspired to keep moving forward.” She remains an active speaker, recently headlining the 2025 MLK Convocation to discuss the intersection of civil rights and mental wellness.
David Feherty (Golf)
With 10 international wins and a successful second career as a commentator, former pro golfer David Feherty has lived a full life alongside the challenges of attention deficit hyperactivity disorder (ADHD) and bipolar depression. He views his condition with a unique perspective. “You know, I tell people I don’t suffer from bipolar disorder, I live with it,” he told Rolling Stone. He even credits it for his broadcasting success: “I see from a different side of the street than most people. And I think one of the reasons I got hired to do commentary is the ability to describe something differently.”
Amanda Beard (Swimming)
A seven-time Olympic medalist and former world record holder, swimmer Amanda Beardfaced battles out of the pool that included bulimia, drug use, major depressive disorder, and self-harm. “Some days, it was hard to just get out of bed,” she told esperanza magazine. Her life turned around when she embraced a combination of medication and therapy. Beard has since transitioned into mentorship, returning to the University of Arizona as an assistant coach in 2023.
Clint Malarchuk (NHL)
Former NHL goaltender Clint Malarchuk is best known for surviving a devastating, life-threatening injury on the ice in 1989. Following that incident, he faced a different battle: post-traumatic stress disorder (PTSD), alcoholism, and obsessive-compulsive disorder (OCD). After pulling himself out of a deep depression through medication, talk therapy, and meditation, he found a new calling. “I realize now that playing hockey gave me the platform for my real purpose,” Malarchuk said. “To raise awareness of mental illness, and to help reduce the stigma surrounding depression and anxiety so that no one has to feel alone.”
Kate Nye (Weightlifting)
As an Olympic silver medalist and former World Champion, American weightlifter Kate Nye (Vibert) appeared to have it all — until a diagnosis of bipolar disorder in 2019 revealed that her periods of intense productivity were actually symptoms of hypomania. After realizing that her ability to train on nearly zero sleep was a warning sign rather than a superpower, she sought help to stabilize her mood. She has since become a vocal advocate for athletes, proving that medication does not dull a competitor’s edge. “I felt weak for thinking I needed help,” she admitted to BarBend. “But honestly, it has taken a weight off my shoulders knowing what I have to do to feel like a functioning human being.”
Suzy Favor Hamilton (Track and Field)
Olympic middle-distance runner Suzy Favor Hamilton experienced intense hypersexuality linked to bipolar disorder, as well as acute peripartum depression. She has courageously shared how her condition drove her toward risky behaviors, using her story to demystify the often-misunderstood symptoms of mania. “In my case, my bipolar was driving me toward sex. It could have just as easily been driving me toward drugs and alcohol,” she told bp Magazine. While she has since stepped back from the public eye to live a private life in California, her candor remains a powerful testimony that diagnosis and treatment can provide a path forward.
Charles Haley (NFL)
As the first five-time Super Bowl champion and a Pro Football Hall of Fame inductee, Charles Haley became an NFL icon. However, his post-NFL life was rocky until a 2002 diagnosis of bipolar disorder helped explain years of struggle, including a decade-long battle with substance use. Haley eventually found balance through medication, therapy, and a men’s prayer group. Today, he dedicates his time to charity work and mentoring the next generation of football players.
I’m so proud of each athlete for sharing their story because when we share the stigma lessons.
Melinda
Reference:

Daily Writing Prompt



That is a short sentence for a big answer! I live a laid back life now and the answer is actually shorter than you might expect.
Mission
Stay close to God
Be a good wife
Take care of my physical & mental health
Find joy by looking out the window
Help the charities I work with
Always looking forward to life
Be informed about the world around me
Cut negatives out of my life
Help when you can
Stay true to myself

Melinda

Affirmations That Lift Your Inner Voice — Even on Hard Days
The post talks about how positive thinking and affermations help with Bipolar Disorder, the truth is everyone can benefilt from the post. What we think and say is what our brain believes.
Words — whether spoken or thought — carry incredible weight. They are capable of healing or harming. The unkind phrases people tell themselves so often can easily turn into beliefs, shaping an unfair and cruel view of who they are.
If words hold so much sway, why, then, can’t they be used for good?
What if your words and what you tell yourself hold the key to a better life? Imagine if, instead of riding along with the usual negative stream of consciousness, you said aloud: “I am worthy.” “I have the strength to overcome any challenge.” “I have come this far — I am capable.”
Appropriately termed “affirmations” or “self-talk,” these are positive statements that can help you confront and overcome self-sabotaging and negative thoughts and beliefs. When you repeat them often and believe in them, you can start making positive changes and rewriting your story.
When Brain Chemistry Meets Self-Belief
Most people spend much of their waking time talking to themselves, although they might not always be aware of it. And that internal chatter is much more influential than many realize. Mood is created by the balance of chemicals in the brain — neurotransmitters like dopamine, serotonin, endorphins, and so on.
Yet even your thoughts or self-talk can alter your brain’s chemical reactions, shaping emotions and behaviors. What you say to yourself has real-world consequences.
“What you tell yourself is how you are programming your internal navigation system,” says Jill Sylvester, LMHC, MEd, who has a private practice in Hanover, Massachusetts, and is the author of Trust Your Intuition: 100 Ways to Transform Anxiety and Depression for Stronger Mental Health.
In this way, a person’s inner speech functions much like an internal compass or brain-based GPS. The tone of this self-talk influences our feelings, judgments, self-esteem, and actions — guiding them to move forward, change course, or settle into the status quo.

RELATED: What You Say Shapes How You See Yourself
Sylvester’s metaphor is fitting and raises an important question: If someone isn’t paying attention to their self-talk, who is at the wheel? And where, exactly, are they going?
Repeated often enough, this silent self-address ultimately establishes a person’s default or foundational beliefs about themselves, those around them, and the world in general. So, in a sense, engaging in mindless self-talk is a lot like living on autopilot.
Even so, anyone can take back the controls. That voice in your head, after all, is your own.
The notion of thinking good thoughts is at the center of much psychotherapy, in fact. Reframing your negative thoughts is a powerful way to heal from past trauma. Furthermore, thinking positively to make yourself feel better is not self-deception, says Gregory L. Jantz, PhD, founder of the Center: A Place of Hope, one of the leading facilities for the treatment of depression.
In his book Moving Beyond Depression, Dr. Jantz writes that positive self-talk is “not mentally looking at circumstances with eyes that see only what you want to see. Rather, positive self-talk is about recognizing the truth in situations and in yourself…. [It] allows you to discover the obscured optimism, hope, and joy in any given situation.”
Transforming Thought Patterns for Better Bipolar Management
Lorenzo L. of New York City knows this firsthand. In his youth, Lorenzo struggled with “massive mood swings” that much later would be recognized as symptoms of bipolar disorder. Showing wisdom beyond his years, Lorenzo lifted himself out of depressive states by slowing his breathing and using positive affirmations.
With regular meditation, Lorenzo has learned to quickly identify his state of mind. Once he is fully aware of his current mood, he directs his self-talk accordingly: “When I’m coming down from mania or hypomania,” he says, his mantra is, “‘Don’t doubt yourself today. It’s okay that you don’t feel as joyful or productive today.’”
“When I’m cycling up to mania or hypomania,” he continues, “I say, ‘Try not to get too carried away. Use all of this extra energy for productive and healthy activities.’”
And when he is feeling balanced, he uses positive, encouraging inner speech to continue his sense of stability: “I can sustain this mood for more than this moment or day.”
“Self-affirmations,” Sylvester explains, “are positive statements that put a person in the driver’s seat of their life and create a path from which to grow.”
And grown he has. Working full-time and studying to become a certified public accountant, the 37-year-old Lorenzo credits his healthy mindset to meditation and cognitive behavioral therapy (CBT). With the help of his psychologist, he has solidified his initial forays into mindfulness and self-affirmation into a practical, tried-and-true strategy that improves his mood and alleviates his symptoms.
Train Your Mind to Respond, Not React
When the terrain is rocky and you’re struggling to stick to your wellness plan, positive self-talk can help you persevere by encouraging you to become proactive instead of reactive. In fact, you can harness your inner monologue to promote what psychologists call “self-regulation” — your ability to exert conscious control over emotional and physical responses to external situations.
You can strengthen your self-regulation by consciously distancing your thoughts from your experiences. One way to do this is to switch your self-talk from first person (“I,” “me,” “my”) to third person — using your own name instead.
An older randomized controlled trial found that doing so during times of stress fosters a sense of perspective, with net benefits including decreased anxiety, improved performance, and faster, more complete emotional recovery.
So, if you’re feeling anxious about an upcoming event or want to gain a bit of emotional separation from an experience to change your response, consider replacing “I” with your name when speaking or thinking your affirmations.
How Positive Self-Affirmations Protect the Brain From Stress
In times of overwhelm, it can be helpful to remind yourself who you are and what defines you as an individual. From there, you can make better decisions.
When Cheryl W. M. faces negative thoughts, she tells herself, “I don’t sweat the small stuff.”
By linking her desired mindset to her self-image in this way, she makes it easier to follow through with her goal of not letting minor inconveniences or difficulties become roadblocks.
Cheryl explains that her affirmation “helps to keep me centered and positive.”
Science supports Cheryl’s experience. In one study, participants with high levels of chronic stress showed reduced problem-solving ability. However, those who engaged in a brief self-affirmation activity performed significantly better on challenging tasks than those who didn’t.
This suggests that self-affirmations can protect against the negative effects of stress, such as impaired creativity and problem-solving.
Confirming the importance of linking affirmations to your identity, Sylvester says that empowering affirmations work best when they begin with “I am,” such as “I am true to myself,” “I am capable,” or “I am smart.” Set in the present tense, they “affirm that things are happening in the present, versus in the future.”
This is when first-person self-talk can prove beneficial, eliminating the emotional distance between your identity and what you want to affirm.
Kim S., understands the power of using self-talk in this way. Every time she looks in the bathroom mirror, she tells herself that she loves herself; then she says, “I am surrounded by love. I am strong today. I can make it right now, just for right now.”
In addition to using “I am” statements that focus on the current moment, Kim, who’s in her early sixties, also imagines being surrounded by white, healing light and beautiful hearts. “And if I have to,” she continues, “I repeat this five times per day.”
The Science of the Inner Critic — and How to Overcome It
When you’re dealing with bipolar depression, it might feel inauthentic or untrue to say to yourself, “I am happy” or “I am capable.” Depression feels heavy and can often rob you of the belief that you can get out of bed, continue with your routines, and return to happiness. At these times, it’s essential to remember that your brain is mistaken.
Clinical psychologist and author of Overcoming the Destructive Inner Voice, Robert W. Firestone, PhD, identifies the “critical inner voice” — the stream of negative, self-defeating, and highly critical self-talk — as the “enemy within.” He writes that this enemy can be overcome only by recognizing it and actively working against it.
By distancing yourself from the “enemy within” and aligning with your true identity through positive, emotionally charged affirmations, you can move toward a more balanced and uplifting state of mind.
That sense of control can feel especially empowering when your mood seems to dictate your days.
Because internal self-talk influences both beliefs and behavior, cultivating awareness of that inner voice enables more intentional, affirming thought patterns.
Lorenzo says, “I know it’s difficult. If you’re struggling, there are ways to adapt your lifestyle and cope with difficult emotions. Such as, for me, affirmations and positive self-talk.”
“It’s a journey,” he says, “for sure.”
Self-Talk Alternatives to Support Bipolar Stability
There are many ways to increase your sense of personal power and inject some positivity and affirmations into your daily routine. Here are a few to get you started.
- To start off on the right side of the bed, Eric R., of California, says he uses the song “Beautiful Day” by U2 as his wake-up alarm. “It sets the tone for the day by pointing my thoughts in a good and hopeful direction as soon as I awake.”
- To instill your new habit, link your self-affirmation to an existing routine, like brushing your teeth. That way, as you stand before the bathroom mirror, you can say to yourself, “I am strong.” Then repeat the practice before bed.
- Embrace your creativity and turn your favorite affirmation into a piece of art. Paint, collage, draw, or design it however you wish, then display the final product in a place you see every day.
- Take things a step further and record your affirmations in your own voice (ideally when in a positive or neutral mental state), suggests Connecticut-based clinical psychologist Kristina Hallett, PhD. Tailor the words to what feels true, and later, during trying times, you can listen to your own voice of wisdom and move forward with calm encouragement from the one who knows you best.
Our mental health stays balanced from many forms of help and we need to look at all angles.
Melinda
Reference:
Book Review-Hope and Learning Our Journey with Schizophrenia by Linda Snow-Griffin
I want to say a special thanks to Linda Snow-Griffin for providing me a copy of her book Hope and Learning, Our Journey with Schizophrenia for a review.
Published 2021
Cherish Editions
About the Author
Linda Snow-Griffin, Ph.D. is a retired psychologist. She is the mother of two, stepmother of three adult children and grandmother of sixteen. She has practiced in a variety of settings – college, university and community mental health – and spent the last 30 years in private practice in Cincinnati. Her desire is to provide hope to families coping with mental illness, especially schizophrenia.
Blurb
When her son was diagnosed with Schizophrenia, Linda Snow-Griffin, a psychologist in private practice, felt devastated and overwhelmed. There were thousands of questions going through her mind: How can I help him? What does he need to get better? Will he be able to get better?
Hope and Learning narrates the 20-year journey Linda and her son embarked on, as they navigated their way towards recovery and a better understanding of what it is like to live with schizophrenia.
This book combines personal experience with schizophrenia with substantial data to create a heartwarming and informative resource.
My Thoughts
Linda shares her journey of her son’s diagnosis with Schizophrenia thru her intimate and raw writing. She discovered a journal of her son’s written in high school that set the wheels in motion that changed their life forever and in surprising ways.
I have Bipolar Disorder, which is a serious mental illness, yet I have been around only one person with Schizophrenia and it was during one of my hospital stays. Being around “John” was not scary but he was totally detached, walked the halls constantly talking to other beings who controlled his life. As you can imagine, that was my perception of Schizophrenia. A stigma/myth that Linda changes in this wonderful book.
Her son is highly functioning with medication and even attended college, it was quite difficult and presented some unique challenges when it came to writing his papers but with the understanding of his mother and love of his family, he made it thru. Linda’s book is heart-wrenching, at times it’s hard to imagine how difficult it must have been on a mother and family but what she shows us is love and understanding concurs all.
I am so glad I read her book, my stigma of what Schizophrenia looked like changed and for that I am thankful.
I recommend this book to anyone who thinks they may have or suspect a family member or a loved one has Schizophrenia, you will learn so much and walk away with answers and tools to take on your journey.
Melinda
Repost
How to Handle Disrespect Without Taking It Personally
Bipolar can make disrespect feel overwhelming. Reframing others’ behavior keeps the focus on their actions — not your worth.
Did you know that no one can disrespect you?
That’s right! No one can disrespect us. When we feel disrespected, we’re taking someone’s words or actions personally, and we choose to feel disrespected. We assign to our response feelings like invalidation or disrespect. In actuality, they are not disrespecting us. Here’s why.
You’ve probably heard it before, but it’s absolutely true: People’s actions are a reflection of the person they are. They are projecting their behavior onto us.
Don’t Take Disrespect Personally
Learning not to take things personally is so important to our mental well-being and happiness. When we think people are being disrespectful, invalidating, or rejecting, that’s when we’re taking their behaviors personally and making their behaviors about us.
Another person’s behavior is not about us. It may feel like people are acting a certain way because of us, but the way people act is always about them.
When we feel disrespected, this is our cue to start reframing the situation for clarity and perspective. Instead of taking things personally and feeling bad about ourselves, we need to change our thinking to find perspective, objectivity, and clarity.
Reframe Negative Thoughts for a Healthier Perspective
I used to feel disrespected all the time, like I didn’t matter, and people put me last or trampled my boundaries. We can feel very low and cultivate a lot of negative thinking about ourselves when we have this perspective. This is not good for promoting a solid sense of self, healthy self-esteem, or positive self-image.
We need to protect ourselves from emotional hurt and invalidation. I’ve found that when I can reframe hurtful actions as experiences rather than taking them personally, it helps me cope with people who may be unaware or hurtful.
Not having the situation be about me makes it easier to maintain perspective, distance, and detachment.
How do you do this? Instead of claiming disrespect, detach from that idea and reframe the situation in terms of how the disrespectful person was behaving. Your thought process is no longer, They were disrespectful to me, which hurt my feelings! Instead, it becomes:
- They were being rude
- They were acting like a jerk
- They were being insensitive
- They were being disrespectful
And here’s the important part, … but that is a poor reflection of them and not hurtful to me.Again, the key here is, that’s not hurtful to me.
Why Strong Boundaries Protect Your Mental Health
The most important dynamic in human behavior and healthy relationships is creating and maintaining boundaries, in my opinion. Boundaries allow clarity, perspective, and detachment because they keep us in a safe space and separated from what crosses our boundaries and creates anger or hurt.arated from what crosses our boundaries and creates hurt or anger.
Melinda
Reference:
Top Bipolar Disorder Support Organizations and Resources
Professional support groups and networks play a vital role in addressing challenges faced by those living with bipolar disorder and their families.
Finding the right support can make a world of difference when living with bipolar disorder. National and international organizations offer resources, education, and community — helping individuals and families feel informed, empowered, and less alone.
These care networks — such as peer and professional support groups — create a sense of connection and belonging and provide practical insights for navigating the often complex mental health care system. They also offer valuable tools, such as self-help strategies and lifestyle recommendations, which empower individuals to manage their symptoms more effectively.
In addition to providing support and resources, some national networks are actively involved in research, clinical trials, and the development of innovative therapies.
Here’s a roundup of the best bipolar support organizations contributing to a brighter future for those who live with bipolar disorder or love someone who does:
National Alliance on Mental Illness (NAMI)
The National Alliance on Mental Illness provides a range of programs designed to educate you and your family about bipolar disorder, including a peer-to-peer program specifically for adults living with mental health conditions.
They also feature a helpline on their website that offers free, confidential support, as well as referrals to local services, and guidance from trained volunteers. With local chapters all over the United States, the national organization can provide you with direct assistance, including access to support groups, educational initiatives, and community outreach programs.
As advocates for improved mental health policies, the National Alliance on Mental Illness actively works to enhance access to care, safeguard your rights, and increase research funding. Plus, they share the latest research findings in bipolar disorder management, helping you stay informed and empowered.
The Depression and Bipolar Support Alliance (DBSA)
As a leading national organization specializing in depression and bipolar disorder, the Depression and Bipolar Support Alliance reaches millions of people each year with its extensive selection of resources. A key feature of their support system is the array of both in-person and online support groups, which are led by individuals who’ve had personal experiences with mood disorders. These groups provide a safe and comforting space where you can share your experiences, gain support, and learn coping strategies. And if you’re interested, they also provide training so you, too, can lead support groups and share your experiences with others.
The organization also offers dedicated resources for support partners, families, and friends. They provide an online community where your support network can connect with others in similar situations to exchange advice and gain support.
In addition to these support groups, the Depression and Bipolar Support Alliance has plenty of educational materials to help you better understand your diagnosis, learn about treatment options, and find strategies for maintaining your bipolar stability.
Mental Health America (MHA)
A reliable resource to guide you on your journey with bipolar, Mental Health America offers a wealth of helpful information. This includes detailed insights into symptoms, understanding the diagnosis process, exploring various treatment options, and practical strategies for day-to-day coping.
Through their website, they offer various tools, including online screening options, to help you identify potential bipolar symptoms, insightful articles about the mood disorder, and hosting educational webinars and podcasts.
Understanding the value of shared experiences and community in managing bipolar disorder, Mental Health America promotes its peer-support platform, Inspire. They also conduct public awareness campaigns to help reduce stigma and advocate for research to enhance our understanding and management of this diagnosis.
International Bipolar Foundation (IBPF)
A valuable support, the International Bipolar Foundation provides a range of educational tools, including informative webinars and detailed blogs to help you — and your loved ones — understand and manage your condition more effectively. If you’re newly diagnosed, they offer a free book to guide you through this journey.
Recognizing the importance of having people around who understand what you’re going through, the foundation maintains a list of support groups worldwide. One of their main goals is to help you connect with these groups and mental health professionals, ensuring you can always find the help you need.
In collaboration with global organizations and experts, the International Bipolar Foundation is dedicated to advancing research to improve our knowledge and treatment of bipolar disorder. They’re also active in raising awareness and reducing stigma through various campaigns, promoting greater societal understanding and acceptance. For anyone in a crisis, they list international suicide hotlines.
American Psychiatric Association (APA)
Dedicated to promoting mental health through research, education, and advocacy, the American Psychiatric Association offers valuable resources for individuals with bipolar disorder and healthcare professionals. They create guidelines that doctors use to diagnose and treat bipolar, ensuring that you’re getting care based on the most current knowledge and research.
They also educate psychiatrists and health providers about the latest findings and treatment methods for bipolar disorder, which helps keep your health team updated and well-equipped to support you.
The association also conducts research and advocates for policies and funding that improve mental health care. This work can lead to a better understanding and treatments for bipolar disorder in the future. You can find informative articles, webinars, podcasts, and guidelines for diagnosis and treatment, all aimed at increasing understanding, reducing stigma, and improving overall care. If you need to find a psychiatrist in your area, consider trying their Find a Psychiatrist tool.
Mayo Clinic
This top U.S. hospital provides personalized care and support for people living with bipolar disorder, which includes everything from diagnosis to treatment. Mayo Clinic’s team of specialists, including those from their Department of Psychiatry and Psychology, work together to create a treatment plan designed specifically for you. This could include medications, therapy, lifestyle changes, or a mix of these.
Mayo Clinic provides educational resources to help you better understand your condition, manage your symptoms, and make informed decisions about your treatment. Plus, they offer support services like stress management assistance and help with any related school or work challenges.
They also have a comprehensive outpatient evaluation and treatment program at the Mayo Clinic Depression Center, along with the Mood Disorders Unit and the Mayo Mood Clinic.
And as part of their ongoing efforts to improve bipolar management, Mayo Clinic conducts research, which means you’d have access to the latest treatment options and may even be able to participate in clinical trials.
National Institute of Mental Health (NIMH)
The National Institute of Mental Health — part of the world’s largest medical research organization, the National Institutes of Health — plays a significant role in supporting you or your loved ones.
A rich source of information about bipolar disorder, they maintain an extensive collection of educational materials on their website, providing in-depth insights into the symptoms, causes, diagnostic process, and treatment methods related to the disorder.
The institute invests in research and clinical trials to improve how we diagnose and treat bipolar disorder, and evaluate new treatment possibilities. They also collaborate with other organizations to raise public awareness about bipolar disorder and reduce its stigma. This helps everyone, from the general public to healthcare professionals, to better understand and respond to the complexities of this mood disorder.
Additional Mental Health Associations and Organizations
The following additional organizations spread awareness and understanding about bipolar disorder, the treatment of clinical depression, and mental health, in general. If you seek additional information about bipolar disease and depression treatment for yourself, a child, or loved one, we encourage you to explore these websites:
United States
- American Academy for Child and Adolescent Psychiatry • aacap.org
- America Foundation for Suicide Prevention • afsp.org
- American Psychiatric Nurses Association • apna.org
- Brain & Behavior Research Foundation • bbrfoundation.org
- Bring Change 2 Mind • bringchange2mind.org
- Families for Depression Awareness • familyaware.org
- The National Federation of Families • ffcmh.org
- Juvenile Bipolar Research Foundation • jbrf.org
- National Council for Mental Wellbeing • thenationalcouncil.org
Canada
- Canadian Mental Health Association • cmha.ca
- Canadian Psychiatric Association • cpa-apc.org
- Canadian Association for Suicide Prevention • suicideprevention.ca
- Mood Disorders Society of Canada (MDSC) • mooddisorderscanada.ca
- Partners for Mental Health • partnersformh.ca
Melinda
Reference:

Happy Birthday Daddy 1940-1992
The morning after you killed yourself, we went to secure the house. I knew immediately you suffered slowly. Among the papers, trash, and clothes and I found your lockbox. The divorce paperwork to my mother, every card I gave you as a child. I found the pad you were writing on. Your Bible on the coffee table, dried tears as you were reading Job in the Bible.
The note had 11:30 a.m. written in the corner. I could see you called your best friend and the phone number to a suicide line. There were words and a drawing that made no sense. Granny paralyzed, crying, asking why. The house ransacked, nothing anything made sense to her.
Dirty dishes piled high, nothing in the refrigerator, how did you live like this, how long? You phoned me several times in the months before your death. Delusional and highly paranoid each time. Someone was tapping your phone, they were trying to get you and the rest I could not understand, you were already gone. As much as I hated you, I cried, begged you not to kill yourself, trying to reason with him that Granny would never be the same. I paid your bills for months. You weren’t in touch with reality.
The outcome will not change if determined. I knew you would take your life and told no-one. I’ve wondered what went through your mind in the hours doodling to writing the note, then killing yourself. I received the call at 10:00 p.m., Gramps said your dad has done away with himself. I called right back to see if you were dead or going to the hospital.
The boxes of cassettes next to your bed, taking months to listen to. You were mentally ill, not under the care of a Psychiatrist, no medications. Your temper went 1-10 in seconds, obnoxious, loud, racist, screaming, out of control.
You had hit the bottom and I didn’t know because we were estranged,
I’ve experienced being suicidal more than once, God and my husband saved me. If you are thinking about suiside, call your Psychiatrist right away or go to closet hospital, be open with your doctor and follow all medications instructions, these actions may save your life. I’ve stayed in Psychistratic Hospitals multiple times, I had 21 ECT Treatments, and I feel no shame. My mental heath is critical to living a balanced life.
I think of you one day a year.
Melinda
Reposted

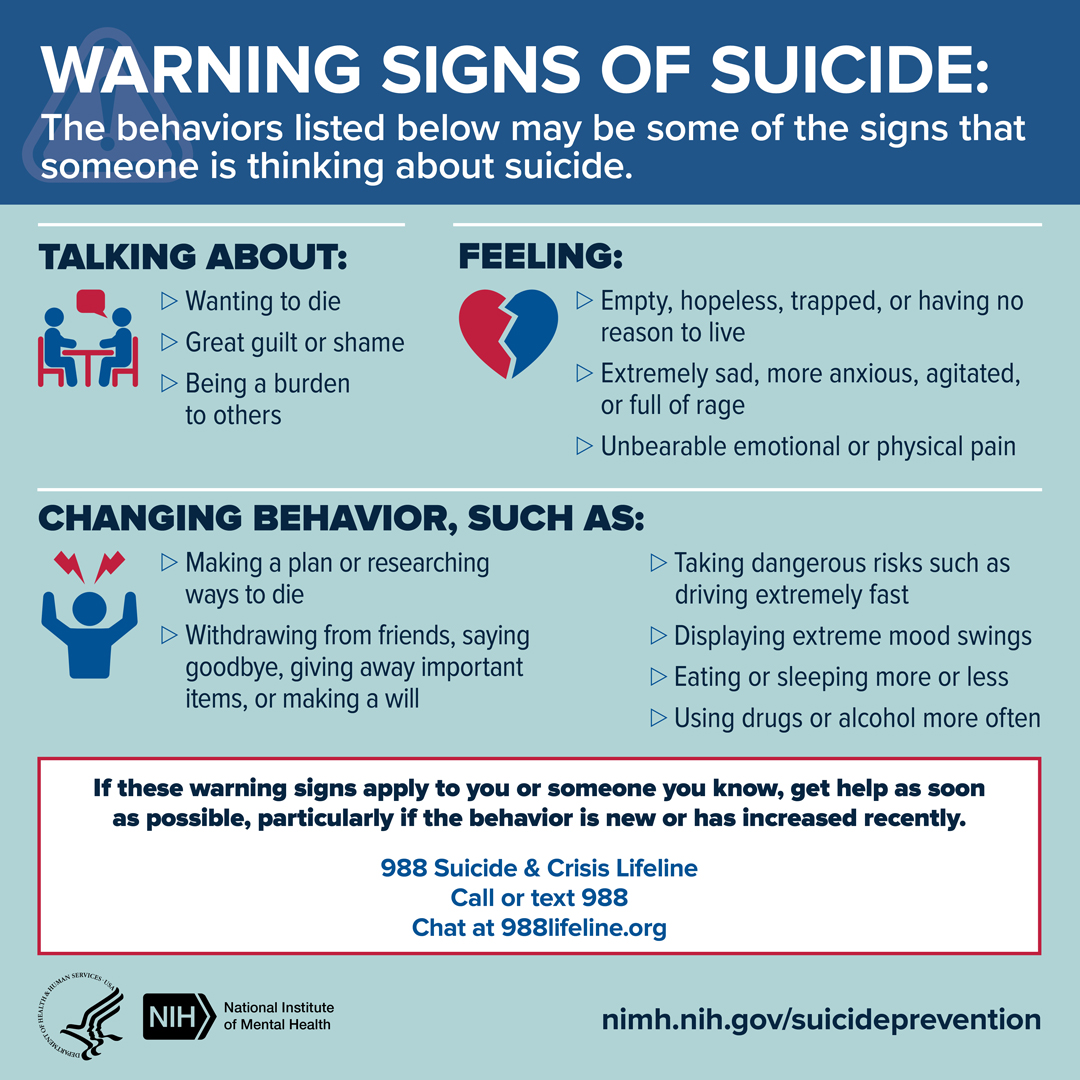
Would You Recognize The Signs That Someone May Be Contemplating Suicide?
Years ago my father’s roommate committed suicide in his bedroom. The signs were clear but my father had no idea. The roommate woke up one morning and mowed the yard, cleaned the house, he returned everything he had borrowed including money owed. He then went to his bedroom and didn’t come out for hours. For reasons unknown to me my father went to check on his gun and it was missing. He knocked on the door repeatedly with no answer. Growing concerned he called the police, the moment the police breached the door the gun went off.
Being familiar with the signs that someone may be in a mental health crisis may save their life, the key is understanding the signs and knowing how to approach the conversations. This is not an easy task and often you will not be let in. That should not stop us from trying. This is a very fragile time and it takes great empathy, patience, and understanding to help someone in crisis. This is not a short-term, wham-bang fix and doesn’t involve your ego.
These are warning signs shared by The National Institute of Mental Health.
In the post How To Start A Conversation About Suicide, Jeremy Forbes has done a great job in his TED Talk video, check it out.
I hope you or someone you care about doesn’t ever reach the point of planning suicide, please reach out or be the person who tries hard to help.
Melinda

Suicide, What’s Left Behind?
This is a previous post I feel is important to shine a light on for Mental Health Awareness Month.
Some states like Colorado have what’s called a Red Gun Law. It basically allows someone who is concerned that a person may harm themselves or others to go before a judge and if warranted, have their weapons taken away for 30 days. This type of law could save many lives, in that 30 days, you might be able to get your loved one or friend the help they so desperately need.
5/30/21
Melinda

My father committed suicide in 1992 after a long struggle with mental illness, he was 52 years old. This post isn’t about how to prevent suicide, or that it’s preventable, this post is about what is left behind after a person commits suicide.
September is Suicide Prevention Month and I’ve struggled with what to write. I do believe strongly that as a society we have to talk about suicide. As much as I advocate for everything I believe in suicide is something so personal to me that it’s different. It’s not the stigma, I don’t care what anyone thinks about my father’s death. It’s that in order to prevent suicide you have to start so far in advance of the person wanting to commit suicide.
My father abused me and we were estranged from the time I was a teenager. When I lived with my father I knew he was emotionally unstable but I was a kid and had my own problems. After 14 years my father calls me and starts talking about suicide. About how he can’t work, how he doesn’t have any money, and on and on.
The daughter and human in me responded, I was heartbroken, in shock, felt responsible and started paying his bills, sending him money and we talked all the time. He constantly talked about people bugging his phone, and people following him. I didn’t realize at the time my father was delusional.
I continued to beg him every time we talked to not kill himself, to think about my granny, his mother who would be devastated. I talked and pleaded for months. Begged him to go to the doctor. I did what I could.
I got a call late one Sunday saying “your father did away with himself” from my gramps. I was in such shock I called right back and asked was he dead or on the way to the hospital. No, he’s dead.
Here are a few things I learned after my father died.
He had been in a downward spiral for years by looking at his living conditions. He had boxes and boxes of cassette tapes by his bed, recordings he had made. I remember him talking about someone bugging his phone so I listened to every one of those tapes several times. There was nothing on most of them, some were recordings of my father talking on the phone. Some were just noise or his breathing. My father was delusional.
I could go on and on but there are a few takeaways.
One of the most difficult things you have to deal with in a suicide death is a closed casket funeral. You can’t see their face and say goodbye so there is an unmet emotional void that never goes away.
I did everything within my power, my dad was a grown man. A man with his own free will. I could not make him go to the doctor for help. There wasn’t a Gun Law in Texas where you could call the police and they would come out to take away a gun. There may not be one now.
I felt unbearable guilt, the pressure of the weight of thinking I could have prevented my granny’s pain was so much I drank myself crazy.
What I did learn from his death as we had the same mental illness, Bipolar Disorder, and I was 75% more likely to commit suicide because my father had. I took that information and I found the best Psychiatrist I could. He is still my doctor today and has saved my life many times.
You can’t stop someone from killing themselves if they are determined. They will find a way now or later.
What we can do is look for signs early in life and during a crisis to see if a person needs help and guide them in that direction. If you’re a parent you have much more control when your child is younger.
The key to preventing suicide is to bring all the emotional damage to the surface to be dealt with and treat mental illnesses with the help of a Therapist & Psychiatrist. I will also add that if you’re inclined you can push for laws that allow the police to be called and for them to take the gun away for some period of time. Each state is different. You can also push for stronger gun laws if that is your wish.
It took me many years to grieve my father but I have reached the other side. You can too.
Melinda
Repost
Mental Health Awareness Month
Mental health is wealth, especially during Mental Health Awareness Month, which is celebrated in May. The stigma around mental health and treatment has long existed, even though this has started to change. Still, people hesitate to seek help or even talk about it with their loved ones for fear of being judged and facing unnecessary backlash. Simple logic dictates that if we are hurt anywhere, we must seek treatment to get better. This applies to both our mental- and physical well-being. While Mental Health Awareness Month is celebrated in the U.S., a more universal day is also celebrated by the WHO on October 10, and it is known as World Mental Health Day.
What To Do When You Need Help
When living with a mental health condition or facing a mental health concern, it’s common to feel like no one understands what you’re going through. But many people overcome the mental health challenges they face. You aren’t alone – help is out there, and recovery is possible.
IF YOU ARE IN CRISIS: Text “MHA” to 741741 or call 1-800-273-TALK (8255) to reach a trained crisis counselor 24/7, 365 days a year. Spanish speakers: 1-888-628-9454. Deaf & hard of hearing: TTY users, use your preferred relay service or dial 711 then 1-800-273-8255
- Use our interactive help-finding tool
- Need to talk to someone? Learn about warmlines
- Time To Talk: Tips for Talking About Your Mental Health
- How to Talk to Your Parents About Mental Health
- Preparing to Share: Talking About Hard Topics
- Self-Help Tools
- Types of Mental Health Professionals
- Choosing a Provider
- Questions to Help QTBIPOC Find Affirming Mental Health Providers
- Working with a Provider
- Finding Therapy
- Find an MHA Affiliate
- Finding Support Groups
- Finding In-Patient Care
- Finding Other Local Services
- Paying for Care
- Complementary and Alternative Medicine for Mental Health
My Mental Health
I was diagnosed with Bipolar Disorder when I was 19 years old but didn’t take it seriously until my father committed suicide in 1992. After a few doctors who gave me way too much medication to work, I found my current doctor.
He’s a Psychopharmacologist and I’m so lucky to have found him. A Psychopharmacologist goes through additional training on top of being a Psychiatrist. One of the most important reasons to see one is if they understand the brain better and which medicine will interact with the part of the brain affected. It takes a lot of the guesswork out of what type of medication you need for your specific symptoms.
If I could make one parting suggestion, it would be to include a loved one in all of the appointments with your doctor. To make sure my husband understood what I was going through and felt it was best to hear it from the doctor’s mouth. It’s been a lifesaver.
Melinda
References:

5 Things I Didn’t Know About Taking Mood Stabilizers
Written by Sally Buchanan-Hagen
Mood stabilizers help keep my bipolar symptoms in check, but they still affect some areas of my life in unexpected ways.
In a previous blog, ‘6 Things I Didn’t Realize About Taking Antipsychotics’, I wrote about some of the impacts that taking antipsychotics can have on your life. But I don’t just take antipsychotics for my <a href=”http://DON’T GIVE UP, MARY! I have had so many bad days, weeks, months, and years even, but when you stick it out, things always get better–sometimes much better than you ever imagined. I encourage you to contact the SUICIDE PREVENTION LIFELINE at 1-800-273-8255. They also have an online chat here: http://chat.suicidepreventionlifeline.org/GetHelp/LifelineChat.aspx. I’ve been in that space before, Mary, and it gets better. I PROMISE! Depression tricks us into believing the world is better off without us, but I PROMISE YOU, THE WORLD IS BETTER OFF WITH YOU IN IT! Please stay…and please stay in touch. bipolar disorder. I also take mood stabilizers. I have been taking mood stabilizers since my diagnosis, but it took two years to get the combination right.
I now take two different mood stabilizers and am happy to say that I am euthymic. Although I experience few side effects from mood stabilizers, taking these medications still impacts some areas of my life.
In a previous blog, 6 Things I Didn’t Realize About Taking Antipsychotics, I wrote about how antipsychotic medications have affected my life. But antipsychotics aren’t the only medications I take for bipolar disorder — I also take mood stabilizers.
It’s worth noting that while mood stabilizer is a commonly used term among clinicians, it’s not an official classification of medication. For bipolar disorder, this category typically includes anticonvulsants and lithium.
1. Tremors
In the beginning, the tremors caused by my mood stabilizer really bothered me. I was on such a high dose of one particular medication that I had to choose between managing my maniaor dealing with wild tremors. It was frustrating, but at the time, the higher dose was necessary to keep my symptoms in check.
I remember being a student nurse on my mental health placement and meeting a young man my age who was on the same mood stabilizer. His tremors were so severe that they made daily tasks — eating, brushing his teeth, writing, brushing his hair, and even getting dressed — incredibly difficult. It took him so much effort just to do things most of us take for granted.
I had no idea then that, just a few years later, I would be struggling with the same challenges — while also trying to write a thesis and work as a nurse in the emergency department. The tremors exhausted me, and I was embarrassed by them. What was hardest was that I couldn’t play the piano or cello, something I truly love. On top of that, the constant tremors felt like a visible reminder that I had bipolar disorder.
Every time my dose was lowered, I would become elevated. During a particularly severe manic episode, I was prescribed an additional mood stabilizer. That second medication, combined with my original one, finally helped keep my mania at bay. More importantly, it allowed me to reduce the dose of my first mood stabilizer without destabilizing my mood. As a result, my tremors are now very mild.
It’s important to point out that the tremors caused by mood stabilizers are different from tardive dyskinesia, a potential side effect of antipsychotics. While both involve involuntary movements, they have different causes and feel distinct from one another.
2. Thirst
Need I say more? Mood stabilizers make you really thirsty. As I mentioned in my previous post, antipsychotics can cause a very dry mouth. Combine that with the thirst from mood stabilizers, and it’s not exactly a pleasant experience.
3. Regular Blood Tests
Some mood stabilizers can make you toxic if they’re over the therapeutic range. To measure this, routine blood tests need to be taken as the level of medication shows up in the blood. I don’t know how many blood tests I’ve had since commencing mood stabilizers, but there have been lots.
When first starting on mood stabilizers, blood tests have to be done very frequently while the dose is titrated up to a therapeutic range.
When I’ve been hospitalized for mania, I would get a blood test every morning. Once the optimal dose has been established for the individual, the blood tests become less frequent, but levels still have to be monitored. I usually get blood work done every two months, but if my dose changes, testing ramps up again.
When that happens, my Saturday morning routine begins with a trip to the local pathology clinic and for a blood test. Fortunately, I don’t mind needles, but I can see how this could be a real challenge for someone who does.
4. Fluctuating Blood Levels
Sometimes, the levels of mood stabilizers in my blood fluctuate. I can always tell when they get too high: I struggle to concentrate, I feel weak, my tremors worsen, and I experience nausea, dizziness, and hot-and-cold flushes.
The first time this happened, I had no idea what was happening to me. I was studying in the university library and seriously considered asking a colleague to take me to the hospital. I didn’t — but looking back, I probably should have. It happened a few more times before I finally made the connection that my medication levels might be too high. Blood tests confirmed it, and my psychiatrist adjusted my dose.
Now, it doesn’t happen often, but when it does, it’s always when I’m dehydrated — which makes sense since dehydration can increase blood levels. Because of this, I have to be extra careful when exercising or on hot days. If my levels spike, it can completely wipe me out for a day or two.
5. Minimal Side Effects
Aside from toxicity — which is extremely serious and requires immediate medical attention — I’ve been surprised at how few side effects I experience from mood stabilizers, especially compared to antipsychotics.
When my tremors were at their worst, I wouldn’t have said this, and I know not everyone has the same experience. But of the three types of medication I take for bipolar, mood stabilizers are the ones I prefer. I owe my quality of life and mentally healthy mind to them.
Sally lives in Victoria, Australia. She was diagnosed with bipolar disorder two years ago when she was 22, however she has been dealing with extreme moods since she was 14. When she experienced her first episode of depression, she was too embarrassed to get help even though she knew that something was wrong. Throughout high school she battled depression after depression, each one getting worse. At university she continued to have depressive episodes and when she wasn’t depressed she was extremely happy, incredibly driven and unusually energetic. Everyone thought this was her normal mood, herself included and so the elevated times went unnoticed. The turning point was in her final year of university when she was referred to the university counsellor. She was diagnosed with depression but after many failed treatments she saw a psychiatrist who diagnosed her with type II bipolar disorder. However that quickly turned into a diagnosis of type I bipolar disorder after a psychotic manic episode. She is currently completing her honours degree in nursing and works as a nurse in the emergency department. She blogs for The International Bipolar Foundation and has written for several publications. She also volunteers for a mental health organization where she delivers presentations about mood disorders to high school students. Although relatively new to this world, she is passionate about mental health promotion and thoroughly enjoys writing about mental health.
Melinda
Reference:

How Can You Measure Stress?
Excessive stress is associated with health complications. Are there ways to accurately measure stress levels?
Although stress is a natural and inevitable part of life, many people feel that they’re experiencing excessive stress levels.
However, there’s no objective way to define “excessive stress.” Many people find it hard to express or quantify their stress.
There are a few methods for measuring stress. These look at certain biomarkers — in other words, physiological responses — to assess how your body responds to stress.
How can you measure stress?
There are two components of stress:
- Stress triggers: the factors that cause stress
- Stress response: how you respond to stress triggers on an emotional, biological, or cognitive level
When we talk about measuring stress, we tend to be talking about measuring triggers or responses. Measuring stress triggers can include taking stock of the major life changes you’ve been under.
However, everybody responds to triggers differently. Events that might be very stressful for one person can be easily manageable for the other.
The following ways to measure stress look specifically at measuring your stress response. These methods of measuring stress look at your body’s physiological responses. They record stress biomarkers such as your heart rate and brainwaves to assess how stress affects your body.
Heart rate variability (HRV)
Heart rate variability (HRV) analysis is a common way to measure stress. It involves recording the variation in time between consecutive heartbeats. In other words, it doesn’t just look at how fast your heart is beating, but how the time period between heartbeats changes.
HRV is controlled by your autonomic nervous system (ANS). The ANS includes your sympathetic nervous system — responsible for fight-or-flight response — and your parasympathetic nervous system, which takes charge when you’re relaxed.
When you’re chronically in fight-or-flight mode, your ANS is unbalanced. This imbalance can show up in your HRV. HRV is lower when you’re in fight-or-flight mode and higher when you’re in a calm state. High HRV is associated with stress resilience and improved cardiovascular health.
A healthcare professional can check your HRV via an electrocardiogram. Personal wearables, such as chest strap monitors, can also measure HRV.
Brainwaves
Electroencephalography (EEG) measures brainwaves. Research suggests that brainwaves can be an accurate way to measure stress response.
In particular, a 2020 study found that alpha asymmetry — an imbalance in alpha brainwave activity on different sides of the brain — could be a potential biomarker for stress.
Mental health practitioners who use neurofeedback can measure brainwaves and train the brain with positive feedback when the EEG finds that treatment goals are being met.
Hormonal testing
Two hormones associated with stress are adrenalin and cortisol.
When you’re stressed, your body will produce adrenalin to give you energy to handle your stressor. It’s a part of the fight-or-flight response, and it’s why you might feel restless when anxious.
In times of stress, your body also produces cortisol, which assists with the fight-or-flight response. Cortisol is a hormone produced by the adrenal gland.
Cortisol is also involved in regulating:
- blood sugar
- inflammation
- metabolism
Your cortisol naturally ebbs and flows during the day. Neither cortisol nor adrenalin is “bad,” but when cortisol is chronically high, it can harm your health. For instance, it can lead to the following:
- acne
- difficulty concentrating
- fatigue
- headache
- high blood pressure
- irritability
- mood problems
- muscle weakness
- weight gain
Lab tests can assess your cortisol levels via urine or blood samples. You can purchase home cortisol testing kits, which usually involve testing cortisol through urine.
The Perceived Stress Scale (PSS)
The Perceived Stress Scale (PSS) is a questionnaire that was developed in 1983. It’s used to assess the amount of stress that you feel you’re under.
Unlike the above-mentioned methods of measuring stress, this tool relies on your own perception of your stress. The questions don’t focus on the events you’re currently experiencing, but your emotional and mental state.
It could be helpful to use the PSS to check in with yourself. It’s available in PDF format.
What are stress trackers?
There are at-home devices that claim to track stress. Usually, these devices track stress by measuring your heart rate and heart rate variability. Many fitness trackers, including smartwatches and chest strap monitors, have stress analysis features.
Are wearable stress trackers accurate? It’s not easy to say. There’s a lack of research into whether these are accurate. However, because these trackers only use one variable — typically your heart — they don’t give a complete picture of your body’s stress response.
What are “normal” stress levels?
Stress is a part of life, and it’s natural to feel stressed from time to time. However, excess stress can be harmful to your health.
When is stress considered excessive? There’s no objective answer to this question. However, if you’re experiencing physical symptoms of stress, or if you feel unable to relax, it may be an indication that you should speak with a healthcare professional.
Similarly, if you feel like you can’t cope or feel overwhelmed most of the time, you might benefit from speaking with a doctor or a therapist.
Symptoms of unhealthy stress levels
The symptoms of high stress levels can vary from person to person.
The symptoms can include:
- acne
- anxiety
- chronic pain
- depression
- difficulty with sleep
- digestive issues
- fatigue
- frequent illness
- headaches
- irritability
- abdominal pain
- weight gain
Although these issues can be caused by other factors, it’s worth speaking with a doctor or a therapist if you believe that stress is causing physical or emotional symptoms.
Tips for managing stress
There are a number of ways to manage stress in a healthy way.
- Try exercise: Find a form of exercise or movement that you enjoy. Yoga, in particular, is associated with stress reduction, but other forms of exercise can also be helpful.
- Practice deep breathing exercises: Research from 2018 suggests deep breathing can activate your parasympathetic nervous system, putting you in a relaxed state.
- Limit screen time: Excessive screen time can harm your mental and emotional health, according to 2018 research. Try to find breaks throughout the day to walk away from your screens.
- Spend time with others: Research from 2020 suggests that spending time with others can help you feel less lonely and stressed. If you don’t have loved ones nearby, join classes, religious services, or meetup groups to get a regular dose of human interaction.
- Try meditating regularly: Research shows that meditation can lower stress and improve overall well-being. If you’re not sure where to start, try a guided meditation.
- Spend time in nature: Being in nature can reduce stress and improve your emotional state, according to 2020 research. Try walking in a local park or natural space, taking up an outdoor sport, or simply eating a meal outside every day.
- Find support: If a particular stressor feels difficult to cope with, consider joining a relevant support group. For example, if you were recently bereaved, a grief support group might help you process your emotions.
If you’re often stressed, you might find it helpful to speak with a therapist. Anybody can benefit from quality therapy — it can help you build resilience to stress and process stressful events in a supportive environment. If the cost therapy is a concern for you, consider other affordable therapy options.
Let’s recap
Stress is a natural part of everyday life. Numerous methods of measuring stress, such as heart rate variability analysis and hormonal testing, could help you find out whether you’re excessively stressed.
However, you don’t need to measure your stress levels in order to justify reaching out for help. If you feel that you could benefit from handling stress better, consider speaking with a therapist or using stress management techniques to improve your well-being.
Melinda
Reference:
https://www.healthline.com/health/stress/stress-measurement?utm_term=roundup&utm_source=Sailthru%20Email&utm_medium=Email&utm_campaign=fibro&utm_content=2025-03-04&apid=36735751&rvid=7f053d6ecf820dccd09e4914833cbd49bdfe95bb517404ee9b41601767d1bace#ways-to-manage-stress
What’s Up With Me
I have been battling depression for several months. I have Treatment Resistant Biplor Disorder. What that means is many medications don’t work on me, or if they do, they stop working at some point. I have been dealing with this up and down since 1992.
One of the medications I started in the Spring, which was working wonders, stopped working. I’ve been working closely with my Psychiatrist to change doses, but nothing is working. He increased the dose today on one of my medications, and I’m always positive it will work. My fingers are crossed.
I’m sure you’ve noticed I have been posting less; I can’t wait to get back to myself.
If your medications stop working, don’t abandon your medications, call your doctor and get the attitude that the next drug will work. You can’t do it alone.
Melinda
Looking For Answers
feeling down
looking for answers
nowhere to go
no joy or fun
waiting for things to change
grey skies every day
know there is hope
the sun will shine
I am blessed
Melinda

February Awareness Days & Months
I’ve included a link below if you would like to see the complete list.
American Heart Month
Black History Month
National Cancer Prevention Month
Teen Dating Violence Awareness and Prevention Month
World Cancer Day 4th
Safer Internet Day 8th
National Donor Day 14th
International Childhood Cancer Day 15th
Random Act of Kindness Day 17th
Day of Remembrance 19th
World Day of Social Justice 20th
National Eating Disorders Awareness Week-Last week of February or the first week of March
You can find the complete list HERE.
Melinda
Reference:
https://www.goodgoodgood.co/articles/february-awareness-days-months

Bipolar and Binge Eating: How I Broke Free
Medically Reviewed by Allison Young, MD
Last Updated: 5 Nov 2024
I tamed my intense cravings and calmed my binge-eating habits to help keep my diet — and my bipolar moods — in balance.
My co-worker carefully extricates her lunch from the toaster oven. The slice of leftover pizza, cheese dripping over its edges, smells divine. She observes me plopping frozen spinach, grilled chicken, and a splash of tomato sauce into a microwave-safe casserole dish and says, “You’re so good. I wish I could eat like that.”
“It’s easy to be good when you’re afraid of passing out over your keyboard from low blood sugar,” I reply to excuse my freakishly healthful lunch. I explained to her that maintaining a good diet keeps my moods in check and would go beyond the bounds of casual break-room small talk.
The steadier my blood sugar levels throughout the day, the steadier my energy, the more alert I feel, the less anxiety I experience, and the more productive I am. The more alert and productive I am, the better I keep bipolar depression at bay.
Work festivities can be a tad awkward, though. I’ve become adept at resisting temptation when someone brings in a plate of brownies, despite the bewildered urging when I refuse. “You gotta try this. It’s Aunt Bessie’s recipe.” Or, “C’mon, who doesn’t like chocolate?” I try to explain, “I love chocolate. It just doesn’t love me.”
Binge Eating and Bipolar Disorder
I used to be a binge eater, regularly losing and gaining as much as 50 pounds. After getting home from work, I could easily inhale ice cream by the pint or a sleeve of chocolate chip cookies dipped in milk — or both. The sugar was like a tranquilizer for my anxious feelings.
Several months and several dress sizes later, I would restrict my eating to lose the excess weight. I cut and cut and cut calories until I was down to diet soda, French fries, and not much else. But crash dieting crashed me into hypomania. By the time I fit into my skinny jeans, my judgment would be even skimpier.
I finally gave up the hard stuff — chocolate, desserts, anything with white flour — when I was trying to get pregnant. (Who knew that wide swings in weight can throw the reproductive hormones off kilter?) Two kids and an education in nutrition later, my weight fluctuates by a more moderate 10 pounds or so. And as long as I don’t eat sugar, I don’t crave it.
How Stress and Fatigue Cause Carbohydrate Cravings
If only it were just sugar. If I’m not careful, bagels and white bread can just as easily send me to Bingeland.
Stress and fatigue fuel our hunger for carbohydrate-heavy treats. There’s a connection between carbs and the brain’s production of serotonin, the “feel-good” hormone — although trying to piece together exactly how this works makes me remember why I flunked organic chemistry.
Here’s an easier tidbit from bio class: The body turns any carb into glucose, a.k.a. blood sugar, to use as energy. The more quickly carbs “dissolve,” the more quickly glucose gets dumped into the bloodstream. Blood sugar levels spike, and what goes up must come down — leading to lethargy and low mood.
In self-defense, I’ve become a student of the glycemic index. Originally developed to help people with diabetes keep their blood sugar in balance, the glycemic index tells you how quickly glucose levels rise after eating a particular food.
White bread, alas, ranks high on the glycemic index. As a compromise, I end my day with a slice of whole wheat bread slathered with crunchy peanut butter and a smidgeon of strawberry jam.
Finding the Right Eating Habits for Bipolar Mood Management
I live in a rush zone from 5:30 a.m. until I chase my daughter into bed at 9:30 p.m. I chow down a protein bar and travel mug of cold water while driving to the office. I write bits of stories and articles in my head while working out. The drive home doubles as a time to make business and social calls.
PB&J on whole wheat unwinds me. It quells my anxiety about everything I need to accomplish before bedtime, everything I am not going to accomplish before bedtime, and everyone I will let down by not getting to every “to do.”
Of course, it’s possible to find that relaxed, comforted feeling through journaling, writing a gratitude list, meditating, stretching, or walking around the block. When I’m tired, though, it’s much easier to use food to chase away my anxiety. And if I actually kept off that extra 10 pounds, what would I have to whine about?
Maybe that’s the real question I need to ask myself: What am I really hungry for? Understanding my needs and making small adjustments can help me balance eating habits and self-care, supporting a healthier, more stable mood over time.
UPDATED: Originally printed as “My Battle of the Binge”, Winter 2014
I had problems with binge eating when I was younger and always tied it to stress. Now I have a different perspective to mull about.
Melinda

Taking Medication: A Small Price to Pay
by Elizabeth Drucker
Medically Reviewed by: Debra Rose Wilson, Ph.D., MSN, R.N., IBCLC, AHN-BC, CHT
Taking medication every day can be tiring and frustrating. But when it comes to living a healthy life, accepting this support is an invaluable step.
When I was 14 years old, sobbing uncontrollably in classes and during cheerleading practice, a psychiatrist scribbled out a prescription for Prozac. I paced through the aisles of the pharmacy, flipping through copies of Vogue and smelling the bottles of shampoo while I waited for the pharmacist to spill the capsules into a bottle.
I knew something was “wrong” with me, but I wasn’t convinced swallowing these pills could make me feel better. I did know I was sad — so sad that it was agonizing to tumble out of my bed and make my way to the bus stop.
Finding what worked for me
Throughout high school, I cycled through the offices of many different psychiatrists. I was always looking for the next pill that could fix whatever was wrong with me.
After I got over the initial shock of needing to rely on psychiatric medications, I started to see these pills as hopeful objects that would bring me some relief.
Each new psychiatrist and each new medication change brought new hope that I would get better. The doctors were encouraged that we would find the right medication and that my life would become more manageable.
Then, during my senior year of high school, I was diagnosed with bipolar disorder. And with that came lithium, pills that are amazing at evening out my moods. So, now I live the lithium lifestyle.
I have to remain vigilant about what my body is telling me because if the level of lithium in my blood gets high enough, I could get very sick. I’ve spent nights sleeping in emergency room beds because the lithium level became toxic and I needed fluids to rehydrate me.
Even still, there’s no denying that this medication has saved my life.
It’s rescued me from some of the deepest, darkest depressions — those times when I felt so broken and raw that I was not sure if I could go on. Lithium has sucked the depression out of my marrow and allowed me to have more of a life.
It’s clear that I need these chemicals to function. And I have a feeling that I will be taking lithium for a very long time, maybe even for the rest of my life.
But I can handle that. I am just grateful that lithium exists, that I can swallow a few capsules and be back on track to regaining myself.
The ups and downs
However, despite its success, there are some nights when I’m so tired that I’m tempted to go to bed without taking my pills. I don’t want to be reminded that I’m sick and that I’m different from all of my friends. I doubt they’re reliant on pills just to survive.
But then, I see flashbacks: me pacing through the corridors of the psych ward; me standing at the medication counter while nurses pour tablets and capsules into little cups; me rocking back and forth on my bed, hoping that I can somehow get some relief from my depression.
So I stumble to the bathroom sink, fill up a large glass of water, and then bring it to my bed. I spill my cocktail of tablets and capsules onto my comforter and start taking them.
I remind myself that these pills are a collection of chemicals that allow me to function, to get through the day without being interrupted by the manic or depressive symptoms of my bipolar disorder.
Taking pills has become a part of every day. And, for me, every day begins and ends the same way: with me taking the pills my psychiatrist has prescribed to keep my bipolar illness at bay.
Accepting the downsides
I think you know by now that, for me, taking my pills is not optional. The consequences are very real and very scary.
My medication keeps the depression at bay. It keeps me on the other side of that locked psych ward door, a place I don’t want to be. My medication allows me to live just like those who don’t need medication — so I can go to college and even get through grad school.
Even though I know all of this, it doesn’t mean I’m thrilled that I’ll be relying on psychiatric medication for the rest of my life. Of course, I worry about the long-term consequences on my body.
For example, I know that lithium can be hard on the kidneys. The medication that does so much for my emotional state can also make me nauseous with trembling hands. And it’s very embarrassing when I’m at a restaurant with friends and my hands tremble every time I reach over to put some food on my plate.
Someone very close to me passed away because he refused to be treated for his own mood disorder. I think of him when I’m reluctant to take my pills.
I know this person in my life didn’t want to take psychiatric medication because of the stigma of mental illness. I feel it myself when I go to the pharmacy to pick up my lithium. I still whisper the names of the medications I’m picking up so nobody will think I’m “crazy.”
The bottom line
Psychiatric medications are effective. I don’t care if I have to experience side effects because anything is better than depression to me. My pills have given me my life back.
I can’t say it’s easy to manage those side effects when they have me sitting in the emergency room getting fluids, but I don’t want to spend my days in bed, crying and isolated.
Depression is one of the most painful things I’ve ever gone through and I’m so grateful my medications exist to bring me back to the real world. I will keep taking them because I want to feel better, and this is how I can.
The article looks at a person’s life and how they manage their illness and medication. I can say without a doubt, that taking your medication as prescribed is the best way to manage your illness.
Melinda
Reference:

A Day In The Life Of A Latvian Mom Interviews Me
Ilze and I have become fast friends. We share many of the same interests and she’s also very wise. Her posts always entertain or teach me something new. Please overlook the mistake I made when I said “Most of my post…..” I don’t write for sympathy. Thank you Ilze for digging deep and sharing with the community.
#5: From Followers to Friends – Melinda from lookingforthelight.blog

I’m so happy to have Melinda from Looking for the Light as a wonderful supporter in the blogging community. Although we haven’t known each other for long, her kindness, warmth, and genuine encouragement always shine through in her thoughtful comments. If you haven’t already, I highly recommend visiting her blog, where she shares beautiful insights … Continue
Melinda

2024 Must-Read Books on Bipolar Disorder
| Reading memoirs and nonfiction about bipolar disorder helps connect with those living with this brain-based condition, whether you have it or love someone who does. By Natalia Lusinski |
| When it comes to bipolar disorder, sometimes it may be difficult for loved ones to understand what the person is experiencing. While they often view it through the lens of caregiving, they may not grasp the individual’s personal perspective.That’s where these books come in. They’ll help you feel less alone, whether you’re the one who has bipolar or know someone who does, like a friend, your partner, a parent, a coworker, a neighbor, a child, or anyone else in your social circle.We rounded up these 10 must-read books on bipolar from this year, perfect for personal reading or as a thoughtful gift for someone who could benefit from them. |
| 1. Daddy’s Magical Rainbow – Having a Parent With Bipolar DisorderWhen a parent has bipolar disorder, it can be challenging for a child to understand the emotional ups and downs that come with the mental health condition. In Daddy’s Magical Rainbow – Having a Parent With Bipolar Disorder, author Sarah P. Foster aims to help children ages 4 to 11 better understand bipolar, though it’s also intended for readers of all ages.The story follows a little girl whose dad has bipolar disorder. She learns that “it’s the bipolar talking” — helping her realize it’s not her “fault” when her dad acts in certain ways, whether he’s angry, quiet, manic, or experiencing other emotions. Off the page, Foster is a special education teacher with 30 years of experience working with children. She also grew up in a home environment that was affected by mental health challenges. The illustrations add a lot of heart to the story and come with a unique touch. The illustrator, Lucie Pedersen, is only 10 years old, which likely explains why her artwork so naturally draws readers into the narrative. |
| 2. An Impossible Life: A True Story of Hope and Mental Illness An Impossible Life: A True Story of Hope and Mental Illness, by Rachael Siddoway and Sonja Wasden, is an award-winning bestseller highlighting how bipolar disorder can affect anyone — it does not discriminate. The book follows Wasden’s journey after being admitted to a psychiatric hospital — against her will — by her husband and father when she was 35 years old. On the outside, her life seemed idyllic: She was a mother of three living in the suburbs with her successful husband. However, behind closed doors, she was battling with intense symptoms of bipolar disorder, including manic and depressive episodes, as well as delusions. The book offers hope to those living with bipolar or those who know someone affected by it. Since her experience, Wasden has become a dedicated mental health advocate. Oprah Winfrey even participated in one of her virtual mental health book club discussions to help inspire female inmates at the world’s largest women’s prison. |
| 3. The Bipolar Therapist: A Journey From Madness to Love and Meaning The Bipolar Therapist: A Journey From Madness to Love and Meaning was written by Marcia Naomi Berger, LCSW. In this memoir, Berger is open and honest about her time spent in a psychiatric ward, particularly from the unique perspective of being a therapist who became a patient in the psych ward. Like anyone else, she had to confront the stigma and shameassociated with bipolar disorder. Through her story, we learn how this experience ultimately made her a more compassionate therapist. “Marcia Naomi Berger’s first-person account of her journey and transformation is courageous,” states Francis G. Lu, MD, professor emeritus in the department of psychiatry and behavioral sciences at UC Davis, in the editorial reviews. “As she writes, ‘Someone with mental illness is much bigger and more complex than their diagnosis.’” 4. Hogbook and Lazer Eyes Hogbook and Lazer Eyes is a graphic novel memoir by writer, actor, and stand-up comedian Maria Bamford and her husband, artist Scott Marvel Cassidy. The story is based on their unique courtship — told from the point of view of their pugs — and how they met on the dating site OkCupid, using the names “Hogbook” and “Lazer Eyes.” As it turns out, they had more in common than they initially thought: They both have bipolar 2 disorder. Whether you have bipolar or have been (or are) in a relationship with someone who does this heartwarming and funny book is sure to resonate. 5. Devout: A Memoir of Doubt In Devout: A Memoir of Doubt, author Anna Gazmarian not only reflects on living with bipolar 2 disorder but also her struggles with spirituality. Raised in an evangelical household, Bazmarian’s 2011 diagnosis at age 18 led to a crisis of faith as well. Now 31 and living in Durham, North Carolina, where she works as an outreach coordinator for The Sun Magazine, a national literary publication, Gazmarian spoke with bpHope about her memoir earlier this year. “The longer I’ve had my diagnosis, and the longer I’ve sought treatment, the more I’ve learned to cope with having it be only part of my identity,” Gazmarian says, adding that opening up about her bipolar diagnosis and its impact has been a healing process. She hopes her story will inspire others. 6. Bipolar, Not So Much: Understanding Your Mood Swings and Depression Whether someone is newly diagnosed with bipolar disorder or has been living with the diagnosis for some time, this book, Bipolar, Not So Much: Understanding Your Mood Swings and Depression, offers valuable insights. Written by Chris Aiken, MD, a psychiatrist and assistant professor at New York University and Wake Forest medical schools, along with James Phelps, MD, emeritus psychiatrist, Samaritan Mental Health in Corvallis, Oregon, the book draws on their medical expertise to help readers understand the complexities of depressionand how to manage and cope with it. The authors also emphasize that bipolar disorder is nota one-size-fits-all diagnosis. They explore various treatment approaches, acknowledging that different methods work for different people. 7. Be There: My Lived Experience With My Sister’s Bipolar Disorder Be There: My Lived Experience With My Sister’s Bipolar Disorder tells the story of author Linsey Willis, the younger sibling and caregiver to her sister Betsy, who has bipolar disorder. Betsy’s diagnosis at 21, despite being an Ivy League-educated woman, came as a shock and drastically changed the course of her life. The book not only draws readers into Linsey and Betsy’s experiences but also resonates with anyone who has a sibling or loved one living with bipolar. At its core, the story carries an important message of resilience and hope. 8. Living Well With Bipolar Disorder: Practical Strategies for Improving Your Daily Life In Living Well With Bipolar Disorder: Practical Strategies for Improving Your Daily Life, David J. Miklowitz, MD, professor of psychology at the UCLA Semel Institute, offers practical strategies for managing life with bipolar disorder. He addresses common stressors to avoid, how to cope when they arise, and ways to handle mood swings effectively. The book covers a wide range of topics, from managing depression, mania, anxiety, and irritability to navigating daily routines such as sleep, relationships, and work. It also explores maintaining physical health, managing substance use, and making the most of medicationsand therapy for long-term mood stability. “Dr. Miklowitz, an acclaimed authority in the treatment of mood disorders, provides clear and valuable suggestions for how to navigate a seemingly unnavigable condition,” Kay Redfield Jamison, PhD, professor of psychiatry and behavioral science at Johns Hopkins University School of Medicine, writes in an editorial review. 9. Crazy… Or Something Else Entirely: A (Mostly) Secret Journey With Bipolar Disorder Jillian Dumond’s Crazy… Or Something Else Entirely: A (Mostly) Secret Journey With Bipolar Disorder is a heartfelt and humorous memoir that offers a candid look at how bipolar disorder has impacted her life, particularly in areas like dating and relationships. Written in a conversational style, Dumond invites readers into her world, sharing personal experiences that are both relatable and engaging. What makes the book even more compelling are the contributions from her family and friends, offering insights into bipolar disorder from a caregiver’s perspective. Through these multiple viewpoints, the book not only provides a deeper understanding of living with bipolar but also highlights the importance of support and empathy from loved ones. 10. The Social Rhythm Therapy Workbook for Bipolar Disorder The Social Rhythm Therapy Workbook for Bipolar Disorder is written by Holly Swartz, MD, professor of psychiatry at the University of Pittsburgh, with a foreword by Ellen Frank, PhD, distinguished professor emeritus at the same university. In this workbook, Dr. Swartz explains how social rhythm therapy can help individuals with bipolar disorder reset their internal body clock, or circadian rhythm. By stabilizing daily routines and rhythms, this approach can reduce bipolar symptoms, lower stress, and support better mood management. The book offers practical tools for applying these strategies in everyday life to promote emotional stability. ABOUT THE AUTHOR Natalia Lusinski Natalia Lusinski is an editor and writer for bpHope and a wellness and lifestyle writer and editor, covering everything from health to travel to personal finance topics. Her work can be seen in several publications, including Business Insider, Yahoo, Forbes, Insight Timer, and the L.A. Times. She spent several years living abroad and is currently working on a travel/grief memoir. (If anyone happens to be in Portugal, she’d love a pastel de nata.) Back in L.A., she runs a popular pizza Meetup and is still trying to find her favorite slice. Her list looks very interesting and helpful. Melinda |
10 Phrases Nobody With Bipolar Disorder Wants To Hear
Medically Reviewed by Allison Young, MD
Last Updated: 31 Jul 2024
Understanding the impact of your words can make a significant difference. Discover more thoughtful ways to express yourself and create a more caring environment.
Words have immense power. They can uplift and encourage but also wound deeply, often without the speaker even realizing it. This is particularly true for individuals living with bipolar disorder, for whom certain phrases can be not just unhelpful but profoundly hurtful. While some of these comments might seem innocuous or well-meaning, they often reflect misunderstandings about the nature of mental health conditions.
These phrases wouldn’t just be hurtful to someone with bipolar disorder; they can be upsetting to anyone, as they often invalidate feelings and experiences.
The goal isn’t to police language but to encourage awareness and empathy. Many in our community have shared that specific comments, though well-intentioned, can worsen their struggles. Understanding why these phrases are hurtful helps us become better allies and offers support that truly helps.
Here are 10 of the most common and hurtful things people with bipolar disorder have heard:
1. ‘Snap Out of It’
This phrase implies that managing bipolar disorder is simply a matter of willpower, which dismisses the complexity and challenges of the condition. Bipolar disorder is a serious mental health condition that involves severe mood swings, including manic and depressive episodes. Suggesting that someone can “snap out of it” minimizes the profound impact these episodes can have on a person’s life. It also ignores the necessity of medical treatment, therapy, and lifestyle changes to manage the disorder effectively.
A more supportive approach would be acknowledging their struggle and asking how to help, such as, “I can see you’re going through a tough time. How can I support you?”
2. ‘Everyone Has Mood Swings Sometimes’
Comparing typical mood swings to the extreme highs and lows of bipolar disorder minimizes the severity of the condition. Mood swings in bipolar disorder are not just simple changes in emotion; they can be intense and debilitating, affecting every part of a person’s life, from their relationships to their ability to function day-to-day. This comparison can make someone with bipolar disorder feel misunderstood and isolated.
Instead, try expressing empathy without comparison: “I can’t imagine how hard this must be for you. I’m here to listen if you need to talk.”
3. ‘You’re Just Being Overly Dramatic or Emotional’
This can be particularly hurtful as people with bipolar disorder may react strongly due to their condition, and being told they’re overreacting can feel invalidating. Such a statement dismisses their genuine feelings and experiences, which are influenced by their brain-based disorder. It’s essential to recognize that their reactions are not within their complete control.
A better way to respond would be to validate their feelings: “It seems like this is really affecting you. How can I help?”
4. ‘I Wish I Was Manic so I Could Get Stuff Done’
This comment trivializes the manic episodes of bipolar disorder, which can involve risky behaviors, sleep problems, and impaired judgment, not just increased productivity. Mania is not simply a burst of energy; it can be destructive and dangerous. You might inadvertently romanticize a very challenging aspect of the disorder by saying this.
A more compassionate approach would be to ask how they are managing their symptoms: “It must be exhausting dealing with mania. What helps you cope?”
5. ‘Maybe You Should Pray More’
While spiritual practices can be a source of comfort for some, suggesting that prayer alone can manage bipolar disorder dismisses the need for medical treatment and professional support. Mental health conditions like bipolar disorder typically require a combination of medication, therapy, and lifestyle adjustments.
A more helpful comment would be: “I hope you find comfort in your faith, and I’m here to support you in whatever way you need.”
6. ‘You Don’t Seem Like You’re Bipolar’
This is along the same lines as “You seem so normal.” This statement can make someone feel like their struggles are being dismissed or that they are being judged for not showing visible signs of their condition. Bipolar disorder doesn’t have a “look,” and many people work hard to manage their symptoms and appear outwardly stable. It’s essential to recognize that internal experiences can differ greatly from outward appearances.
Instead, you might say: “I admire how well you manage your condition. How are you really feeling?”
7. ‘Why Can’t You Just Be Happy?’
Suggesting that happiness is simply a choice overlooks the complex factors that influence mood in bipolar disorder. Happiness is not a simple decision for someone with a brain-based disorder; it can be influenced by connections between brain cells, life circumstances, and other factors beyond their control. This question can feel dismissive and make the person feel blamed for their condition.
A more supportive statement would be: “I’m sorry you’re feeling this way. What can I do to help?”
8. ‘Have You Tried Just Not Taking Your Meds?’
This can be dangerous advice, as managing bipolar disorder often requires careful medical supervision, and abruptly stopping medication can have serious consequences. Medications for bipolar disorder are usually carefully prescribed and monitored by a healthcare provider to manage symptoms and prevent an episode. Suggesting someone stop their medication can undermine their treatment plan and pose significant risks.
Instead, express support for their treatment plan: “I hope your treatment is helping. How are you finding it?”
9. ‘You Just Need to Exercise More’
While exercise can be beneficial for mental health, suggesting it as a cure-all solution minimizes the complexity of bipolar disorder and the need for comprehensive treatment plans. Exercise is part of a broader treatment strategy that includes medication and therapy.
Instead of suggesting a simple fix, acknowledge the complexity of the condition: “Exercise can be helpful. What else is part of your treatment plan?”
10. ‘You’ve Got It So Good, Why Are You Depressed?’
This minimizes the person’s feelings and implies that their life circumstances should prevent them from feeling depressed, which is not how bipolar disorder works. Depression in bipolar disorder is not about having a bad day; it’s a severe symptom that can occur regardless of external circumstances.
A more empathetic response would be: “I know things might look good from the outside, but I understand that doesn’t change how you feel. How can I support you?”
UPDATED: Originally posted November 27, 2016
CAREGIVERS, FAMILY, FRIENDS, RELATIONSHIPS, STIGMA
ABOUT THE AUTHOR
Tanya Hvilivitzky has spent more than 30 years in the communications field — a career that has included stints as an investigative journalist, managing editor for a lifestyle and wellness magazine, corporate communications director, and researcher/writer. She has been with bpHope (and bp Magazine) since 2016, serving in roles such as features editor, interim editor, and, currently, senior editor. She has been devoted to mental health awareness since she was the editor of Schizophrenia Digest in her early days, and now with a particular focus on highlighting the complexities of bipolar disorder through compassionate, service-based journalism. As an award-winning writer/editor, Tanya received the Beyond Borders Media Award for her 2012 investigative exposé about human trafficking for Niagara Magazine. Her work on this critical topic also earned the Media Freedom Award “Honouring Canada’s Heroes” from the Joy Smith Foundation to Stop Human Trafficking.
Melinda
Reference:
ADHD Awareness Month
My father had ADHD and being a teen in his days must have been horrible, the medication of choice was tranquilizers. He wasn’t diagnosed until he was a teen but the minute he moved out he stopped the medication and I can see why. The issue is he didn’t go back to the doctor as medication evolved and it affected his relationships.
I also believe that doctors are too fast to diagnose ADD & ADHD. One important factor is that Medical doctors don’t have the training to diagnose and are often the ones who diagnose first. To have a proper diagnosis, you need a Psychiatrist, and do the testing for an official diagnosis. My last Psychiatrist listed me as ADHD, with no testing, and no conversation, it just showed up on my chart. I would not be ashamed if that was a proper diagnosis but it wasn’t. My proir Psychiatrist of 32 years never once mentioned it. It’s one of the reasons I no longer see my last Psychiatrist.
—
Every October is Attention Deficit Hyperactivity Disorder (ADHD) Awareness Month, an occasion to raise awareness and support for those with ADHD.
In the United States, about 8.4% of children and 2.5% of adults have ADHD, making it one of the most common mental health conditions. Symptoms of the condition include ongoing patterns of:
Inattention, which means a person may find it challenging to focus or follow directions, but usually, it may not occur due to rebellion or challenges with understanding something.
Hyperactivity, which is when a person may feel the need to move constantly, even when it may be inappropriate for the situation.
Impulsivity, which means the person may have difficulties managing impulsive behavior and considering the long-term consequences of those actions.
Many people may have occasional difficulties paying attention, sitting still, or managing impulsive behavior. But for someone with ADHD, these difficulties tend to occur more often, which may affect how they perform certain daily activities.
During ADHD Awareness Month, communities shed light on this condition and rally to support those who have received diagnoses.
This information from the National Institute of Health has great resources and there may be more that I didn’t read on another page.
Where can I learn more about ADHD?
Free brochures and shareable resources
- Attention-Deficit/Hyperactivity Disorder: What You Need to Know: This brochure provides information about ADHD in children, teens, and adults, including symptoms, diagnosis, causes, treatments, and resources to find help for you or your child (also available en español).
- ADHD in Adults: 4 Things to Know: This fact sheet provides information about ADHD in adults, including symptoms, diagnosis, causes, treatments, and resources to find help for yourself or someone else.
- Shareable Resources on ADHD: These digital resources, including graphics and messages, can be used to spread the word about ADHD and help promote awareness and education in your community.
Multimedia
- Mental Health Minute: ADHD: Watch this short video to learn about ADHD.
- NIMH Expert Discusses Managing ADHD: Learn the signs and symptoms of ADHD and how it is treated as well as tips for helping children and teens manage ADHD symptoms.
Federal resources
- Centers for Disease Control and Prevention (CDC) : The CDC offers fact sheets, infographics, and other resources about the signs, symptoms, and treatment of ADHD in children.
- MedlinePlus : This resource from the National Library of Medicine provides information, research, and resources on ADHD and ways to learn more (also available en español ).
Research and statistics
- Journal Articles : References and abstracts from the National Library of Medicine’s PubMed
- Statistics—ADHD: Statistics on the prevalence and treatment of ADHD among children, teens, and adults
Last Reviewed: September 2024
There is so much information available so don’t put off learning about ADHD, it could help direct your child or yourself to the proper help.
Melinda
Reference:
https://www.healthline.com/health/adhd-awareness-month#history

NAMI Texas Advocacy Newsletter
The newsletter talks about how to vote, the players in Texas who are up for election, and additional resources. Sometimes these newsletters publish a link, not sure why I can see the content but WordPress turns it to a link. Please click on the link or copy in paste on your computer to read. This message is important to all Texans.
October 2024
We are less than one month out from General Election Day! It is critical that Texans get out and vote as policymakers elected in 2024 will make major decisions regarding individuals and families affected by mental health conditions. Furthermore, exercising your right to vote ensures representation, the individuals we elect will be our voice at the local, state, and federal levels. When you participate in elections, we hold our elected officials accountable for their actions and decisions. Additionally, voting has the ability to drive social change as voters have the opportunity to advocate for policy reform and issues that are important to us. Finally, voting promotes equality, providing an opportunity for all citizens to have a say in the decision-making process. Important Dates: General Election Day: Tuesday, November 5th, 2024 Early Voting: Monday, October 21st-Friday, November 1st, 2024 Last day counties can receive mail-in ballot requests: Friday, October 25th, 2024 Find out what’s on your personalized ballot by checking out Vote411.  Get involved & encourage others to do so too! The NAMI Texas team encourages you to check out NAMI National’s #Vote4MentalHealth campaign webpage where you can pledge to vote for mental health, learn more about why mental health is more than a single policy issue and several ways to get engaged. Furthermore, the campaign provides resources like finding your voting options, requesting an absentee ballot, and planning to vote. #Vote4MentalHealth Videos Check out this video that highlights the importance of voting in all elections, from those at the White House to local school board elections. Additionally, watch this educational video on how votes for education, economy, and healthcare all impact mental health! Please note: #Vote4MentalHealth is nonpartisan – the NAMI Alliance will never tell people what party or candidate to vote for; instead, it focuses on understanding how every person’s vote impacts mental health. NAMI Texas Voter Guide: Additionally, check out NAMI Texas’ General Election 2024 Voter Guides! The Policy Team has collected information from Texas candidates on various mental health topics. This guide can be used to help you gather information regarding where candidates stand on various mental health systems and what they hope to improve upon if they are elected. Please note, that all candidates were contacted and only those who responded are in the guides. Texas House of Representatives General Election Voter Guide Texas Senate General Election Voter Guide |
Let’s get out and vote!!!!!!! Our voice needs to be louder than ever if policy changes are going to happen.
Melinda


National Suicide Prevention Month
The topic of suicide is not the easiest conversation but one that is often important. One misconception is that only people with mental illness commit suicide and that is far from the truth. People commit suicide for many reasons and they are deeply personal, like the person dying of cancer and in immense pain or someone who has a chronic health condition that is debilitating and greatly limits their ability to take care of themselves or leave the house. There are many reasons people get deeply depressed and look to suicide as a way out. Yes, there are people with mental illness who commit suicide but I think the media has a role in highlighting these deaths over the other circumstances. Those types of stories get more traffic and unfortunately, keep the stigma alive.
Although I feel that you can’t stop a person determined to commit suicide, I do believe the strategies used long before the person reaches that point are critical and can save lives.
Here are the CDC’s recommended strategies to prevent suicide
Strengthen economic supports
- Improve household financial security
- Stabilize housing
Create protective environments
- Reduce access to lethal means among persons at risk of suicide
- Create healthy organizational policies and culture
- Reduce substance use through community-based policies and practices
Improve access and delivery of suicide care
- Cover mental health conditions in health insurance policies
- Increase provider availability in underserved areas
- Provide rapid and remote access to help
- Create safer suicide care through systems change
Promote healthy connections
- Promote healthy peer norms
- Engage community members in shared activities
Teach coping and problem-solving skills
- Support social-emotional learning programs
- Teach parenting skills to improve family relationships
- Support resilience through education programs
Identify and support people at risk
- Train gatekeepers
- Respond to crises
- Plan for safety and follow-up after an attempt
- Provide therapeutic approaches
Lessen harms and prevent future risk
- Intervene after a suicide (postvention)
- Report and message about suicide safely
See Suicide Prevention Resources for articles and publications about prevention strategies for suicide.
Need help? Know someone who does?
Contact the 988 Suicide and Crisis Lifeline if you are experiencing mental health-related distress or are worried about a loved one who may need crisis support.
- Call or text 988
- Chat at 988lifeline.org
I have a serious mental illness, Treatment-Resistant Bipolar Disorder and it can be difficult to manage, it takes a village and commitment on my part to keep my mood stable. The first time I tried to commit suicide was at nine years old, it wasn’t due to my illness it was due to the abuse and living in a house with Domestic Violence. It’s hard to watch your mother get beaten to a pulp almost daily even if you hate her. I’ve tried many other times and got close a few times all for the same reason.
The suicidal thoughts and plans from my Bipolar Disorder are different in that the Black Dog can sneak up on you slowly and before you realize it, you’re down the rabbit hole. Fortunately, I’ve been aware enough to call my Psychiatrist and to tell my husband. That’s when I know it’s time to visit the Psych Hospital. There are many treatments Psychiatrists can use to help you when you’re at the bottom and can’t see the light. The technology has advanced so much even since I had my first ECT treatment, for which I’ve had 27, six last summer. The great news is there are other treatments now that are proven and cause less memory loss.
My father committed suicide in 1992 and it came as no surprise in that he told me for months he was going to kill himself. My father and I were estranged since I was a teen and yet he started calling me months before he died. I begged, cried, tried to reason, and even paid his bills for a couple of months thinking the financial relief might help. The bottom line is, you can not stop someone who is determined to commit suicide. My father was mentally ill and refused to go to the doctor, his decision and he fell too far down to even think of living. The key point here is that you can’t stop someone who is determined to commit suicide. I’m not saying don’t try, try like hell but you have to accept the facts and not carry the quilt around.
I carried that quilt for seven years before I sought out a Therapist to help me work through the pain and childhood trauma. I didn’t seek help for my Bipolar Disorder until after my father’s death. While reading about his disorder I read that 75% of children of parents who commit suicide will as well. That woke me up! It wasn’t easy, in fact, it was very difficult because medicine after medicine didn’t work. It was very frustrating but I had the greatest Psychiatrist and we finally found a protocol that worked. It was tweaked many times because the medications would stop working but he had enough history on me that he could react quickly to build another protocol. This rebuilding of medication protocols is a part of my disease and one I’m used to. After 32 years, I’m better equipped to explain what is happening and how I feel which helps get to a better treatment faster. Even though I talk quite a bit about mental illness there are many reasons people without a mental illness commit suicide.
The only words of wisdom I can part with is to pay attention to a person’s change in behavior, often you will see one. One example is, hurriedly someone gets all their chores done, cleans the house, and returns items borrowed. That’s called getting things in order and is a good indicator they plan to commit suicide. I encourage you to read more about why people commit suicide to acquaint yourself, just make sure you don’t over-focus. The last thing you want to do is push hard on someone who is feeling suicidal or has a plan. It’s a natural reaction, I know but they can shut you out.
If you are feeling suicidal or have questions you can reach out to these resources:
Emergency Number
911
Veterans Crisis Line: 1-800-273-8255 press 1
Suicide Prevention Lifeline: 1-800-273-TALK (8255
http://www.suicidepreventionlifeline.org
National SuicidePreventionLifeline.org 1-800-273-TALK (8255) Press 1, Veterans Crisis Line USA Press 2, Se Habla Español LifeLine Chat
Suicide & Crisis Lifeline: 988
National Domestic Violence Hotline: 1-800-799-7233
National Hopeline Network: 1-800-SUICIDE (800-784-2433)
Crisis Text Line: Text “DESERVE” TO 741-741
Lifeline Crisis Chat (Online live messaging): https://suicidepreventionlifeline.org/chat/
Self-Harm Hotline: 1-800-DONT CUT (1-800-366-8288)
Essential local and community services: 211, https://www.211.org/
American Association of Poison Control Centers: 1-800-222-1222
National Council on Alcoholism & Drug Dependency Hope Line: 1-800-622-2255
National Crisis Line – Anorexia and Bulimia: 1-800-233-4357
GLBT Hotline: 1-888-843-4564
TREVOR Crisis Hotline: 1-866-488-7386
AIDS Crisis Line: 1-800-221-7044
Veterans Crisis Line: https://www.veteranscrisisline.net
TransLifeline: https://www.translifeline.org – 877-565-8860
Melinda
Reference:
6 Rap Artists Who Have Opened Up About Their Bipolar Disorder
Last Updated: 16 Sep 2024
These rappers have shared their struggles with bipolar disorder, bringing awareness to their experiences within the rap community and beyond.
In recent years, it has become more common for celebrities to talk openly about their mental health, and several well-known rappers have significantly contributed to this conversation over the years. Despite facing controversies and navigating the complexities of the public eye, these artists shared their own stories about living with bipolar disorder. Their honesty helps others feel less alone and sparks more conversations about mental health.
Whether discussing their experiences in interviews or incorporating them into their lyrics, these rappers contribute to a more extensive dialogue about mental health. They’re helping to shift perceptions and encourage a more accepting and informed conversation around bipolar disorder. Here are six rappers who are part of this critical conversation:
1. Krizz Kaliko
Samuel William Christopher Watson, who performs under the stage name Krizz Kaliko, is an American rapper, singer, and songwriter. He has made significant contributions to the music industry as a longtime collaborator with Tech N9ne, another artist from his hometown. Initially signed to Strange Music, the label co-owned by Tech N9ne, Kaliko established his own label, Ear House Inc., in 2021.
Diagnosed with bipolar disorder, Kaliko has openly addressed his mental health struggles in his music. Specifically, in his album Genius, he delves deep into his experiences on the track titled “Bipolar,” where he raps and sings about the challenges of living with the condition.
Beyond his music, Kaliko has spoken candidly about his use of psychotherapy and anti-anxiety medications as part of his ongoing effort to maintain emotional and mental stability. His openness about his struggles inspires and supports others facing similar battles.
2. Ye
Kanye West, now known as Ye, has been vocal about his bipolar disorder, referring to it as his “superpower.” He first revealed his diagnosis around the release of his 2018 album Ye, where he used his music and public statements to address the complexities of living with the condition. The album’s cover features the phrase, “I Hate Being Bipolar; it’s Awesome,” reflecting his struggle with the extremes of the disorder.
Ye has continued to discuss the impact of bipolar disorder on his life, comparing it to having a “sprained brain” and emphasizing the importance of proper care, even though he has openly struggled with staying on medication consistently.
In recent years, Ye has also opened up about the paranoia and erratic behavior that accompanies his manic episodes. He has criticized how people with mental health conditions are often mistreated, both by healthcare systems and society at large, contributing to the stigma around mental illness.
3. Charles Hamilton
Charles Eddie-Lee Hamilton, Jr., a Harlem, New York City native, is a recognized figure in the hip-hop community as a recording artist and record producer. His album The Pink Lavalamphas been hailed as one of the standout underground hip-hop releases of its time.
In a candid interview with Billboard, Hamilton discussed the personal struggles he faced due to his undiagnosed bipolar disorder. He described a period of intense isolation, where distrust of others led him to confine himself to his home, dedicating his time solely to music production as a way to combat his depression. “I just didn’t trust anybody,” he admitted. “I didn’t leave my house; I just made music all the time. I was fighting depression — I shut myself in.”
Over the years, Hamilton has been open about his mental health journey, using his platform to raise awareness about bipolar disorder and the importance of mental health care. His career has seen various ups and downs, including a brief retirement in 2016 followed by a return to music with new projects that reflect his ongoing battle with mental health and his resilience in the face of adversity. His candidness about his struggles has not only helped to destigmatize mental health issues among musicians and fans but also resonated with audiences worldwide.
4. DMX (Dark Man X)
Earl Simmons, known professionally as DMX, was a prominent figure in the music and acting industries, rising to fame in the late 1990s. His raw and emotional lyrical content often reflected the personal pain and struggles associated with bipolar disorder, which was especially evident in his groundbreaking album, It’s Dark and Hell Is Hot.
DMX’s bold and unique contributions significantly shaped the music landscape, particularly as the only artist to debut his first two albums at number one in the same year.
His music not only captivated fans but also offered a visceral insight into his battles with mental health. Until his passing in 2021, DMX’s powerful voice in music and film left a lasting impact, celebrating the profound expressiveness of his work.
RELATED: 20 Musicians You May Not Know Have Battled Bipolar Disorder
5. Adam Steven Deacon
Adam Steven Deacon, an English talent celebrated as a film actor, rapper, writer, and director, shot to fame with his performance in the British film Kidulthood and his directorial debut, Anuvahood. In an interview with the BBC, Deacon discussed his initial fears that his bipolar disorder might derail his career. He described the condition’s impact, saying, “Bipolar life has two speeds: One minute, it’s all too fast. The next, everything becomes so slow that I can’t cope.”
This candid account of his daily struggles sheds light on the complexities of living with this brain-based disorder. Deacon has since learned to embrace and manage his conditioneffectively. His story of resilience and adaptability provides hope and insight, encouraging others to navigate similar challenges.
6. Yo Yo Honey Singh
Yo Yo Honey Singh, also known as Honey Singh, is a prominent Indian rapper, music producer, and film actor renowned for his contributions to Bollywood music. He rose to fame as one of the highest-paid music producers in Bollywood. But in late 2014, Singh took a sudden hiatus from the public eye, sparking concern among his fans. After a quiet return to the music scene in 2015, he maintained a low profile with the media. It was not until March 2016 that Singh revealed the reason for his 18-month absence: he had been battling bipolar disorder.
Since disclosing his diagnosis, Singh has gradually resumed his music career and has been involved in several new projects, adapting his workload to manage his health effectively. His openness about his mental health struggles has been instrumental in raising awareness and reducing the stigma associated with mental health issues in the entertainment industry and beyond.
Tanya Hvilivitzky has spent more than 30 years in the communications field — a career that has included stints as an investigative journalist, managing editor for a lifestyle and wellness magazine, corporate communications director, and researcher/writer. She has been with bpHope (and bp Magazine) since 2016, serving in roles such as features editor, interim editor, and, currently, senior editor. She has been devoted to mental health awareness since she was the editor of Schizophrenia Digest in her early days, and now with a particular focus on highlighting the complexities of bipolar disorder through compassionate, service-based journalism. As an award-winning writer/editor, Tanya received the Beyond Borders Media Award for her 2012 investigative exposé about human trafficking for Niagara Magazine. Her work on this critical topic also earned the Media Freedom Award “Honouring Canada’s Heroes” from the Joy Smith Foundation to Stop Human Trafficking.
Melinda
Accepting Your Bipolar Disorder Diagnosis
By Donna Jackel
Medically Reviewed by Allison Young, MD
Last Updated: 10 May 2024
Accepting a bipolar diagnosis can be immediate, offering clarity on past experiences, or it may be a gradual process of coming to terms with a lifelong condition.
At age 29, Julie C. seemed to be at an enviable place in life. She had good friends. She had come out as a lesbian and was comfortable with her sexuality. And she had a fulfilling job that took her to far-off places: She was coordinator of a Toronto-based foundation.
That life began to slip away from her in 2007, when she was beset by money and relationship problems. Julie was hospitalized twice, and treated for depression. But her psychologist knew another side of the young woman — the high-energy, high achiever who could sometimes work at a furious pace with little sleep. In 2008, the psychologist told Julie that she believed she had bipolar disorder.
Fearing the Unexpected, a Diagnosis of Bipolar
“I was terrified at first,” Julie recalls months later. “I had this dropping feeling in my gut. All the stereotypes I had about bipolar came flooding into my head. I have a friend who has bipolar, and she has been almost homeless a couple of times, and in and out of the hospital. I thought, ‘Oh my God — is this what my life is going to be?’”
Julie has since accepted her diagnosis. She is stable and feels much better than in the past. She takes her medication daily, maintains a regular sleep schedule, works out, and has improved her eating habits. She still works for the foundation, but is planning to move back to her hometown and work long-distance.
For others, the road to acceptance can be long and circuitous. Peggy M. of Wisconsin has experienced highs and lows since her teens. Although Peggy was diagnosed with bipolar in 2002, acceptance did not come until six years later when she had her first negative work evaluation.
Peggy received a poor rating in several areas; the comment that hurt most was “poor communication skills.” “I have a master’s degree in communications. [The review] was a direct contradiction to what I knew about myself,” Peggy says. “That’s when I finally had to admit it was the bipolar affecting my work.”
Your Journey to Acceptance of Bipolar Is Unique to You
Many factors influence how well a person is able to adapt to bipolar. These include the severity of the illness, level of self-awareness, one’s attitude about mental illness, availability of a support system, and access to quality health care.
Some are able to accept their illness after one or two manic episodes. Others remain in denial for years, burning through relationships, jobs, and money until they hit rock bottom.
“Bipolar is one of the illnesses people have the hardest time accepting,” says Sagar V. Parikh, MD, deputy psychiatrist-in-chief at the University Health Network in Toronto and professor of psychiatry at the University of Toronto.
“Maybe one-third accept the diagnosis right away. At least a third totally reject it, and a third believe it, but when they are better for a while, begin to doubt it again,” explains Dr. Parikh.
“It’s common for acceptance to take years,” agrees Evette J. Ludman, PhD, a clinical psychologist and researcher at Group Health Cooperative in Seattle and coauthor of Overcoming Bipolar Disorder: A Comprehensive Workbook for Managing Your Symptoms and Achieving Your Life Goals.
Fully accepting the diagnosis is “almost like joining the priesthood,” Parikh says. “The commitment to treatment is a major one that involves going to the doctor regularly and paying a lot of effort to regulating one’s lifestyle. It’s not just a commitment to medication, but a way of life.”
In his research, Parikh found that people living with bipolar 2 have greater difficulty acknowledging the diagnosis than do those with bipolar 1, which is typically characterized by clear-cut episodes of mania and depression.
The symptoms of bipolar 2 are more subtle, he explains, making it difficult to perceive the hypomania as a symptom of the mental health condition, rather than part of one’s identity.
“Your highs are mild, your brain is working faster, you have more confidence and energy, you need less sleep — it’s the ideal human condition,” says Parikh. Because hypomania is less obvious than mania, “it is difficult to conceptualize it as an illness,” he adds.
Personal Research, Reflection, and Ultimate Acceptance of the Diagnosis
In his 20 years as a Methodist minister, Ron M. encountered people with bipolar disorder — there was the female parishioner who had threatened him with a knife, and the wild young man who had stripped off all his clothes. Because Ron associated the illness with such extreme behavior, he missed his own symptoms when they began in early 2003. He attributed his racing thoughts, restlessness, and crying jags to depression.
His behavior resulted in Ron being placed on disability leave by his denomination; he began seeing a psychiatrist and a therapist and started taking an antidepressant. Eight months later, Ron was diagnosed with bipolar 2 and prescribed a mood stabilizer.
He continued to tell himself he was “only” suffering from depression, however.
“I was convinced that if I could tough it out, I’d be fine,” he says. “I told myself, ‘There is no way I’m bipolar.’”
During this period, his marriage of 20 years ended. Looking back, Ron says it was this denial that prevented him from getting adequate treatment. Despite his skepticism, Ron began reading about bipolar disorder and keeping a mood chart.
By the summer of 2004, he had accepted his diagnosis. “The research indicated that my moods and cycling were pretty consistent with the disease,” he says.
Since this breakthrough, life has “gotten a lot easier,” Ron says. He is more open-minded about taking medication. And by continuing to chart his moods, he can predict the ups and downs.
“I will have five to seven good days and then I will crash and have about seven to 10 dark days,” he says. “You can almost set your watch by my cycling.”
Meanwhile, a series of changes have enriched Ron’s life. He moved from St. Louis to Tucson to be near family and friends; medication adjustments have brought him greater wellness, and he fell in love and remarried.
“When I grieve for how my life used to be, I remind myself that if it was like it used to be, I would never have met her,” he says of his wife.
Because of his rapid-cycling, Ron, now in his fifties, does not believe he will be able to lead a congregation again. However, he finds great fulfillment in helping others as president of the Tucson chapter of Depression and Bipolar Support Alliance (DBSA).
“I force myself to go to meetings when I’m not feeling good,” he says, “And when I am feeling good, I need to go so I can share with someone to help them in their time of struggle.”
Stigma, Discrimination, and Denial of Bipolar
Indeed, the stigma and discrimination associated with mental illness is a huge barrier to coming to terms with bipolar, consumers and experts agree. It is because there are so many misconceptions and preconceptions about mental illness that Dr. Ludman hesitates using phrases like “accepting the diagnosis.”
“I’m not very fond of labels,” she explains. “Everyone has their own story of what ‘accepting’ [the illness] means. It may mean ‘I’m crazy,’ or ‘No one loves me.’”
Jo R., an executive assistant for an Atlanta-based optometry association, resisted her 1997 diagnosis for eight years. To her, bipolar disorder meant that she could no longer trust her own mind.
“After 36 years of living, I couldn’t think my thoughts were incorrect,” says Jo, who grew up in poverty in the small hamlet of Jasper, Florida. “I was intelligent and had accomplished a lot, so I couldn’t be ‘crazy.’”
Jo told herself that her sleeplessness and psychoses were side effects of her antidepressant. Denial cost her deeply: She lost two jobs, resulting in bankruptcy and the loss of her home. But it was not until she spent a week in a state mental hospital that the reality of her situation fully hit.
“There was a beautiful woman there who yelled and barked like a dog; there was another girl who urinated on herself,” she says. “The people there were ‘crazy,’ and I was among them, so I was one of them. I told the doctor, ‘I’m ready to do whatever I need to do to manage this.’ That’s when I accepted the diagnosis.”
Jo made good on her promise, learning all she could about bipolar and what she needed to do to stay well. Today, she works full-time and has her own apartment. She keeps a mood chart and a journal, exercises, takes her medication, and avoids “toxic” people.
Indeed, Jo is so vigilant about maintaining her downtime and getting enough sleep that friends and family know not to call her after 9 p.m. She carefully tracks her spending, keeping to a strict budget, and recording all her purchases.
“The bipolar diagnosis has been a true blessing,” Jo now will tell you. “Having bipolar forces you to change to be the best you can be … to live a good life.”
Moving Toward Accepting and Embracing Your Bipolar
The first step following a diagnosis of bipolar — even before medication — should be learning about your illness, says Parikh. “It is the single most effective remedy aiding acceptance. You’re not going to follow any treatment plan unless it makes sense to you.”
Mental health experts generally agree that accepting the diagnosis makes it easier to follow a treatment plan. Yet disagreement exists as to how to best approach patients who are in denial. Gary S. Sachs, MD, founder and director of the Bipolar Clinic and Research Program at Massachusetts General Hospital and an associate professor of psychiatry at Harvard Medical School, doesn’t “push acceptance as a requirement.”
“Many patients will be willing to accept some form of intervention if I don’t require that they accept the label as well,” he says.
“Ambivalence about treatment is kind of the norm,” agrees Mark S. Bauer, MD, professor of psychiatry at Harvard Medical School, director of the Harvard South Shore Psychiatry Residency Training Program, and a coauthor of Overcoming Bipolar Disorder.
“Studies show that only 20 percent [of consumers] come to treatment fully on board,” says Dr. Bauer.
Rather than try to convince skeptical patients, Bauer teaches them how to recognize their mood swings, understand how episodes have affected their quality of life, and how to control these patterns. He also helps people “develop a detailed plan for living a full life, based on their values and core goals.”
But others believe that accepting the diagnosis is integral to treating the mental health condition effectively. “By accepting what the problem is and informing yourself about the disease and treatment, you are empowering yourself to control the disease,” says Francis M. Mondimore, MD, assistant professor at Johns Hopkins University School of Medicine’s Department of Psychiatry and Behavioral Sciences and author of Bipolar Disorder: A Guide for Patients and Families.
“My message to people is that we know a lot about how to treat this problem and manage the symptoms,” says Dr. Mondimore. “You need to know all the options so you can make an informed healthcare decision. Once you’ve named something, you’ve got some control over it.”
Lise, of Vermont, grew up around mental illness. Her father died when she was 17, and her late sister dealt with a mental health condition.
“I was always in fear of being like my sister,” Lise admits. A librarian at Norwich University in Northfield, and the mother of three teenage boys, Lise had for years been treated sporadically for depression. Then a 2003 car accident — a drunk driver totaled the car she and her family were riding in — heightened her depression.
Her family doctor switched her antidepressant, and before long, Lise became manic. She left her husband and sons and moved into an apartment. Hospitalization and a diagnosis of bipolar 2 followed.
“At first, I was just dealing with the ramifications of what I had done, and was kind of in shock — how could I lose sight of my kids and my family?”
Then, Lise had to learn to live with a new diagnosis. Instead of the more socially acceptable label of depression, she had a severe, chronic mood disorder. “It was scary, and it made me sad,” she recalls.
In fact, people often “get very caught up in whether symptoms indicate depression or bipolar,” says Mondimore. “What we’re learning about mood disorders is there is a lot of overlap.”
Although sometimes there are discrete manic or depressive episodes, people can also experience mixed episodes, which have symptoms of both.
As time goes on, we probably won’t even have separate categories for depression and bipolar. Instead, there will be a classification for mood disorders.”
Lise found that her family history actually strengthened her resolve to reclaim her life. “I lost my father … and I will not do that to my kids, no matter how hard it is,” she says. “I go get help as soon as I feel those thoughts coming.”
Medication Can Make a Difference in Bipolar Mood Management
Medication adherence is the biggest roadblock to fully accepting bipolar disorder, according to Mondimore. “That is the hardest thing — admitting that you are not always able to control your emotional life,” he says.
But these feelings subside with the support of loved ones and by undergoing psychotherapy, he adds.
Side effects are a more tangible reason people refuse, or go off, psychotropic medication. For example, Jo had to learn to live with a 100-pound weight gain and hand tremors.
For her part, Julie initially refused to take lithium because it was so heavily associated with bipolar disorder. “I had talked myself into thinking I had bipolar-lite — that I had a very mild version of what other people had,” she says wryly. “Friends also told me not to take it — that I could manage without it.”
But then Julie began cycling more noticeably. “One week I would be excited and the next, I would think the world was ending,” she says. “My therapist said lithium would help that.”
It can also be deeply frustrating to accept that medications can only manage, not cure bipolar, Ludman points out.
The notion of having to take pills every day for the rest of her life intimidated Wendy L., of Owensboro, Kentucky, who has “trouble doing anything routinely.” But there was a more basic reason Wendy at first resisted medication: “I liked my manic highs — I felt very productive. I didn’t want them taken away,” she says.
After discussions with her husband, however, Wendy decided that, for his sake, she needed to stabilize her moods. “We’d been married for 30 years and I put my husband through hell those 30 years,” she says.
Diagnosed at age 50, Wendy has gradually learned to live with “flat” moods. “I was used to flying high and feeling all these ranges of emotions, and that wasn’t there anymore.”
Missing the soaring highs and bursts of energy leads many to stop their medication and land back in the hospital. “It’s very common for patients to stop taking mood-stabilizing medication when they begin to feel better,” Ludman says.
Social Support to Stay on Track With Bipolar Treatment
Dr. Sachs believes that having someone in your life to help you stay on track is so crucial for individuals with bipolar that he helps those who don’t have an existing support system to develop one. “Mood disorders include periods when your perceptions are distorted, so the most important thing to include in your treatment plan is a care partner,” he says.
Those fortunate enough to have a loved one willing to join them on the road to recovery travel a less lonely path. “My husband educated himself. We sat down, talked about the symptoms, signs, and different triggers that had happened over years,” says Wendy. “He was willing to work through the changes. He was so accepting of it that it helped me accept it.”
You don’t have to be in a romantic relationship to find support — an understanding boss who lets you come to work a bit later because a new medication is making you sleepy; family and friends who visit you in the hospital; or a relative with bipolar who shares what worked for him — all can contribute to your wellness.
Julie, who was living in a small town when she came out as a lesbian, believes society is more accepting of homosexuality than mental health conditions. “In my office, I don’t care if people know I’m gay,” she says. “The few co-workers who do know about my bipolar will be like, ‘So are your meds working now?’ as if I’ll get on some meds, and then I’ll be ‘normal.’ That’s not going to be it — I’ll have to manage my bipolar — even when I’m well.”
When Julie told her boss she had bipolar, the woman, who is also a good friend, responded: “You are still the same person. Nothing has changed, except that you know something about yourself that can make you feel better.”
UPDATED: Printed as “Accepting The Diagnosis,” Summer 2009
Donna Jackel specializes in mental health, animal welfare and social justice issues. She earned a bachelors degree in journalism at the S.I. Newhouse School of Public Communications at Syracuse University. For 15 years, Donna was a staff reporter at the Democrat and Chronicle, a daily newspaper in Rochester, NY, where she still lives. As a freelancer, in addition to contributing to bp Magazine and esperanza, Donna’s work has appeared in ReWire, The Progressive, Lilith, Texas Monthly, Yes! Magazine, The Chicago Tribune, Bark Magazine, CityLab, Leap Magazine and other national publications. A story Donna wrote about her mother’s (Marie Rogers) service in the British Air Force during World War II was included in the anthology, Before They Were Our Mothers: Voices of Women Board Before Rosie Started Riveting (copyright 2017). In 2019, Donna won an honorable mention in health writing from the American Society of Journalists & Authors for a feature story she wrote for The Progressive about college students who were denied transgender hormone therapy. When Donna isn’t working, she can be found hanging out with her Lab, Bear, horseback riding or catching a movie at the Little Theatre. Her work can be seen at donnajackel.com.
Melinda

How to Tell Others About Your Bipolar Disorder
By
Medically Reviewed
by
Published on September 26, 2023
While some people may not struggle to tell friends, family members, or an employer about their bipolar disorder, for others it can feel very nerve-racking. These 7 tips can help.
At age 31, Julie A. Fast — now a bipolar disorder expert and researcher — was diagnosed with the condition. Later on, she was diagnosed with schizoaffective disorder, bipolar type (a psychotic disorder involving symptoms of both schizophrenia and bipolar disorder).
Bipolar disorder wasn’t entirely new to Fast, now 59, when she was diagnosed. Her partner at the time was diagnosed with the condition in 1994, just one year before.
Still, in her social circles, she found that most people did not know or understand her condition. “I’d go to a party, and maybe two or three people would say, ‘I know of bipolar disorder,’” says Fast, who coauthored the book Take Charge of Bipolar Disorder with John Preston, PsyD.
Because awareness of bipolar disorder and its symptoms is increasing, many people with the condition, like Fast, feel more comfortable sharing their diagnosis with others. “I can deal with whatever happens when I disclose my illness to others,” Fast says. “It will show who can help me and who can’t.”
But some people with bipolar disorder may still feel hesitant to share their diagnosis, in part because of stigma and fear about how others will respond, experts say.
Why Sharing a Bipolar Disorder Diagnosis Can Feel Challenging
Factors like shame, embarrassment, or stigma — negative and often untrue beliefs society holds about someone or something — make some people with bipolar disorder feel hesitant to talk about their condition, research shows.
Many people with bipolar disorder experience a form of stigma called “public stigma,” which is related to how other people view and act toward people with bipolar disorder, according to research published in February 2022 in the Australian & New Zealand Journal of Psychiatry. Public stigma is linked to more anxiety symptoms, worsened ability to function, and problems at work, per the same research.
Although public stigma can come from anyone around them, many people with bipolar disorder experience it from people close to them — family, friends, or even their healthcare providers, per the same report.
Fear of how others may respond as a result of stigma is another potential barrier. “They may worry that disclosure could negatively affect their relationships with friends, family, or romantic partners,” says Leanne Quigley, PhD, an assistant professor in clinical psychology at Yeshiva University in New York City.
Public stigma and how others view bipolar disorder can lead many people with the condition to feel negatively about themselves, according to the aforementioned report.
“[They] may also experience internalized stigmas where they report low self-esteem, low quality of life, and limited engagement in their communities,” says Adrian Jacques H. Ambrose, MD, MPH, the medical director of the psychiatry faculty practice organization at Columbia University in New York City, who treats people with bipolar disorder. This is what’s known as “self-stigma,” per the aforementioned report.
RELATED: A Therapist Speaks: What Is Bipolar Disorder Stigma, and How Can We End It?
When to Tell Someone About Your Bipolar Disorder Diagnosis
The decision about when to share your diagnosis with someone else is very personal. It can depend on the type of relationship you have with the other person and whether they seem to have some sort of understanding of conditions like bipolar disorder.
When It Comes to Your Significant Other or Someone You’re Dating …
For romantic relationships, Fast recommends sharing a bipolar diagnosis as soon as possible. “I don’t really support the idea of getting in a relationship with somebody unless you have fully discussed the impact of bipolar on the relationship,” Fast says.
That’s important because the symptoms can affect the way someone with bipolar disorder thinks, feels, acts, and communicates with their partner, according to the United Brain Association. For instance, during a manic episode, someone with bipolar disorder may experience intense irritability toward their partner or may have a higher chance of engaging in risky behaviors like unprotected sex or heavy spending, which could lead to tension or mistrust in a relationship, per the United Brain Association.
If you haven’t talked about your condition with your partner, it can be difficult for them to know what to say or do to help.
When It Comes to New Healthcare Providers …
It’s also crucial to be up-front about your diagnosis with any new healthcare providers you see, Fast Adds. They need to know about your health history and any medications you take. Research shows that certain medications, such as corticosteroids like prednisone, can trigger mania and psychosis in people with bipolar disorder.
That’s why Fast told her doctors before a recent minor surgery that she was not comfortable being prescribed steroids, which are sometimes used to help reduce inflammation. “When they suggest steroids, and so many doctors use steroids, I explain why I can’t use them,” she says, adding that her doctors were receptive to her needs.
Some antidepressants, such as fluoxetine (Prozac), also trigger mania in people with bipolar disorder.
When It Comes to Your Friends and Family …
When it comes to telling friends and family, it might take you some time to feel comfortable doing so — and that’s okay. Prioritize telling close friends and family members that you interact with frequently and who you feel understand you well — rather than people you rarely interact with, Fast advises.
Before sharing your diagnosis with friends or family, Dr. Ambrose recommends asking yourself the following questions:
- Do you feel ready to share?
- Is there anything pressing or urgent happening that makes it important to tell them sooner rather than later, such as the onset of a mood episode?
When It Comes to Your Employer …
When it comes to your work environment, it’s important to weigh the possibility of discrimination, says Ambrose. You could look to see if the company has in recent years tried to reduce mental health stigma, which research suggests could make the workplacemore welcoming for workers with mental health conditions.
And if you don’t feel comfortable revealing your specific diagnosis, that’s okay. You can still bring a note from your healthcare provider asking for accommodations based on how your mental health condition impacts your functioning, according to the U.S. Equal Employment Opportunity Commission.
7 Tips for Talking About a Bipolar Disorder Diagnosis
If you feel ready to share your diagnosis with someone else, here are seven expert tips to get the conversation started.
1. Prepare Yourself for All Sorts of Reactions
Just as people diagnosed with bipolar disorder may have a range of reactions to their diagnosis, reactions from others can vary, too. “We can allow the other person to ask whatever questions they want, have any type of response that they want,” says Fast.
Although some people may react positively to hearing about your diagnosis, others may react in a negative way. “Remember that your self-worth is not determined by a diagnosis of bipolar disorder or others’ reactions to your disclosure of a diagnosis,” Dr. Quigley says.
2. Talk About How Your Bipolar Symptoms May Affect Others
During a manic episode, some people with bipolar disorder may be more prone to engaging in risky or hurtful behaviors, such as cheating or lying. This can be common for people who are undiagnosed, Fast adds.
Whether you’ve just gotten your bipolar disorder diagnosis or you’ve received treatment for a new mood episode, it could help to reach out to people who may have been harmed by your words and actions during the episode. It could be a message like, “I’d love to talk to you about my diagnosis because I know my behavior impacted you,” says Fast.
But it’s important to recognize that not everyone will want to engage in this conversation, especially if they feel really hurt by actions like cheating or stealing, for instance, Fast adds.
If behavior related to a bipolar diagnosis hasn’t yet come up in your relationship with someone else, the person you’re telling may have questions about how it could affect the relationship in the future. Be prepared to discuss how any episodes could manifest.
3. Have a Summary on Hand
After sharing a bipolar disorder diagnosis, some people may have follow-up questions about your symptoms or, in the case of work, any accommodations you might need. “In certain situations, your loved ones [or employer] may know very little about mental health conditions, so it may be helpful to prepare a short summary about the condition,” Ambrose says.
The summary could be either written or verbal (or both), depending on what you’re most comfortable with.
4. Work With Your Therapist on a Plan to Tell Others
If you feel nervous or worried about sharing your diagnosis with others, your doctor or therapist could help you come up with the best strategy for you for sharing your diagnosis, says Fast. “Share most of your concern and your worries with your healthcare professionals because they’re trained to handle it,” Fast says.
5. Understand Your ADA Rights (and Note That They Vary by State)
While the Americans with Disabilities Act (ADA), which prohibits discrimination against people with disabilities at work and all other areas of life, is a federal law in the United States, some states offer more protections than others when it comes to employment laws related to disability discrimination, says Ambrose.
“Given the complexity of work-related rights, you should learn more about your specific state’s legal statutes,” Ambrose says.
If you’re in an area with less protection, it might be worth talking to a third party, for example your state labor office, about the best approaches for disclosing a bipolar diagnosis at work. State government offices belonging to the U.S. Department of Labor can help you better understand your rights as a worker in the state you live in. The Department of Labor has a directory of state labor offices.
6. Offer Different Information in Different Situations
If you’re only comfortable disclosing the entirety of your diagnosis to some people and not others, that is perfectly fine. “You may choose to discuss certain parts of your experience with bipolar disorder and not others,” Quigley says. “It is okay to maintain boundaries and not share everything.”
7. Give Yourself Grace
It can be difficult to figure out how to tell others about your diagnosis. It’s important to take care of yourself during this time. “It’s even more important to cultivate a sense of empathy and grace for yourself during the process,” Ambrose says.
Julia Métraux
Author
Julia Métraux is a journalist whose work touches on disability, mental health, and chronic illness. She went to the University of California in Berkeley Graduate School of Journalism. Métraux lives with vasculitis, a traumatic brain injury, and hearing loss.
————
I know how hard telling others about your mental illness can be, especially family members. Many family members looked at me differently because they were from a different generation that did not believe in mental illnesses. I did not tell friends or my employers because it wasn’t their business. One of my employers fired me from a high-level job because they found out I had a mental illness, yes I could have sued the billion-dollar company but why go down that multi-year road through the rabbit hole. I caution everyone to think hard before telling your employer, it can be held against you and they can find a way to fire you.
Melinda

12 Celebrity Quotes That Perfectly Describe Life With Bipolar Disorder
By Tanya Hvilivitzky
When famous people share their personal battles with bipolar disorder, it serves as a reminder that no one is isolated in this struggle. After all, bipolar disorder is indifferent to wealth, fame, or success.
It’s easy to believe that celebrities — actors, musicians, or comedians — enjoy lives of perfection. However, what is publicly seen represents just a fraction of their actual lives. The truth is, bipolar disorder doesn’t discriminate. It makes no distinction between a person’s age, gender, race, or bank account size.
So, when stars living with bipolar disorder share their own struggles, it signals to others that they are not navigating the complexities of this brain-based disorder alone, reinforcing the message that, together, managing it is within reach.
Here are personal and powerful quotes from 12 such celebrities:
1. Taylor Tomlinson
It took a little while for comedian Taylor Tomlinson to accept her bipolar diagnosis. She explains to E! News her reaction upon learning about her mood disorder. “I was surprised that I felt embarrassed when I first found out. Because I think I’m very open-minded. I have friends who have bipolar. And you never judge your friends. You never felt like that was a big deal. But then when it’s you, you somehow realize you have all this deeper stuff from when you were a kid.”
2. Cameron Esposito
After telling her fans earlier this year of her bipolar diagnosis, Cameron Esposito, standup comic, actor, and writer, took to her Instagram channel on her birthday in October 2023 to reflect on the year: “… you know what? I’m lucky. I’m lucky that I figured it out. I’m lucky that I had a place to go. I’m lucky that I was enough in my faculties that I was extremely persistent with following up after that experience, and getting my meds and finding a psychiatrist. All that s&*t is impossible and so expensive. I have healthcare coverage; I have insurance. I just want to say to anybody who’s had to navigate this [mental health care] system … you are a hero! Look at you! Look at what you’ve been able to do!“
3. Alan Ritchson
Actor Alan Ritchson, star of Prime Video’s Reacher, was diagnosed with bipolar at age 36. In a February 2024 interview with CBC Radio’s “Q” program, Ritchson explains why he’s been sharing his story to help others: “As much as I would like to ignore that I’m a suicide survivor, if I didn’t share what I’ve learned I feel like my life would be meaningless,” he says. “I’ve always been a happy-go-lucky guy, but once you experience the grip [of depression] — the talons it can sink into you — you realize how sinister this thing is and how out of control the biology can really be for somebody in the midst of it.”
4. Carrie Fisher
“In my opinion, living with manic depression takes a tremendous amount of balls. Not unlike a tour of Afghanistan (though the bombs and bullets, in this case, come from the inside). At times, being bipolar can be an all-consuming challenge, requiring a lot of stamina and even more courage, so if you’re living with this illness and functioning at all, it’s something to be proud of, not ashamed of. They should issue medals along with the steady stream of medication.” — Carrie Fisher, Wishful Drinking, 2008
5. Ye (Kanye West)
As a guest in 2019 on David Letterman’s Netflix series, My Next Guest Needs No Introduction, Ye (Kanye West) uses the term “ramping up” to convey the process of entering a hypomanic or manic bipolar mood episode: “When you ramp up, it expresses your personality more. You can become almost adolescent in your expression. … When you don’t take medication every day to keep you at a certain state, you have the potential to ramp up … and even end up in the hospital.”
6. A.J. Mendez
In an interview with bp Magazine, former pro wrestler A.J. Mendez (AJ Lee) says, “I see bipolar disorder as the gift of extraordinary emotions. It makes me bold, brave, loud, and capable of withstanding whatever obstacles the world throws at me. It has made me empathetic. It has given me a lofty imagination, a belief in the impossible, and has made me confident beyond reason. I was 90 pounds and five feet tall and believed I could succeed in the world of giants … because I didn’t have that voice of doubt holding me back.”
7. Richard Dreyfuss
Richard Dreyfuss has starred in blockbusters like Jaws, American Graffiti, Close Encounters of the Third Kind, and The Goodbye Girl (which earned him an Academy Award for Best Actor). Of his bipolar diagnosis, he says, “No matter what you call it, this is an illness no different from, say, diabetes or asthma — and like those conditions, [it] should be neither ignored nor stigmatized. Feeling ashamed would mean surrendering to someone else’s judgment — an ignorant judgment at that.”
8. Linda Hamilton
The Terminator actress Linda Hamilton uses a holistic health plan to help her stability, with a structured and balanced lifestyle, exercise, and medication. “Exercise is an incredible key to feeling well. But for people with mental illness, taking care of the body is not an automatic thing. The mind is in such chaos, it’s hard to come up with a plan. So, to people like us, it’s more important than ever to follow a regimen.”
9. Maurice Benard
Daytime actor Maurice Benard — who plays Michael “Sonny” Corinthos Jr. on General Hospital — talked with bp Magazine on life with bipolar: “I’ve lived a productive life having bipolar. I’ve talked to people who don’t want to talk about [having bipolar] because it’s embarrassing. I’m proud of it because I know it’s made me the actor I am and the person I am. It’s given me strength. If I can go through being in a mental hospital, and that kind of pain, and that kind of fear, I can do anything.”
10. Maria Bamford
In an interview with bp Magazine’s Melody Moezzi, the comedian Maria Bamford talked about being diagnosed: “I was surprised how prejudiced I was against myself. They tell you it’s the brain chemistry also working its magic, but I was really surprised at how resistant I was to going on a mood stabilizer, taking any time off of work, acknowledging that I needed to be hospitalized. I was just so angry. I didn’t want to go on the meds. It wasn’t until it got bad enough to where I was starting to feel unsafe by myself that I reconsidered.”
11. Stephen Fry
In an interview with bp Magazine, Stephen Fry said of creativity, “It is not a coincidence, it can’t be, that so many comedians suffer from depression. As for whether the hypomanic side of bp can be said to help creativity, I hesitate to say yes because of all those out there living with the disorder who are not in creative industries. … But certainly, the energy, self-belief, exuberance, tirelessness, optimism, and, yes, grandiosity that mark out hypomania can really help one achieve much in terms of writing and creation.”
12. Mariah Carey
In 2018, during an interview with People magazine, Maria Carey spoke about the confusing ups and downs of bipolar disorder: “For a long time I thought I had a severe sleep disorder, but it wasn’t normal insomnia. … I was working and working and working. … I was irritable and in constant fear of letting people down. It turns out that I was experiencing a form of mania. Eventually, I would just hit a wall. I guess my depressive episodes were characterized by having very low energy. I would feel so lonely and sad, even guilt that I wasn’t doing what I needed to be doing for my career.”
UPDATED: Originally posted June 19, 2020
Tanya Hvilivitzky has spent more than 30 years in the communications field — a career that has included stints as an investigative journalist, managing editor for a lifestyle and wellness magazine, corporate communications director, and researcher/writer. She has been with bpHope (and bp Magazine) since 2016, serving in roles such as features editor, interim editor, and, currently, senior editor. She has been devoted to mental health awareness since she was the editor of Schizophrenia Digest in her early days, and now with a particular focus on highlighting the complexities of bipolar disorder through compassionate, service-based journalism. As an award-winning writer/editor, Tanya received the Beyond Borders Media Award for her 2012 investigative exposé about human trafficking for Niagara Magazine. Her work on this critical topic also earned the Media Freedom Award “Honouring Canada’s Heroes” from the Joy Smith Foundation to Stop Human Trafficking.
I dislike what Carrie Fisher had to say. It’s not appropriate to compare an illness to those who fought in Afghanistan and I do not think people with Bipolar Disorder deserve a medal and more medication. My thoughts about her have remained the same, she used her Bipolar Disorder as an excuse for her bad behavior and to make money. My opinion.
Melinda
Denial in Bipolar Disorder: The Manic Fallacy of Wellness
Last Updated: 7 Aug 2024
During my first manic episode, I was convinced I’d finally recovered from my chronic depression. But my therapist saw symptoms of bipolar disorder.
I’m a doctor by training, so you’d think I would have guessed I had bipolar disorder, for heaven’s sake. I certainly manifested every symptom of mania in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), from boundless energy and soaring spirits to severe insomnia.
I should have known something was up when I treated myself to a $4,000 antique French buffet table. (The credit card company considered shutting down my account, but I convinced them that my finances were under control.)
I subscribed to delusions of grandeur, scouring my home for a spot to exhibit the writing award I was guaranteed to win. My sexual appetite spiked to new heights, too (no complaints from my guy on this point).
Friends and Loved Ones Were Baffled by My Behavior
Certainly, my friends and loved ones noticed a bizarre new me bursting onto the scene. One friend, irritated by my self-absorption, said she felt I had come across “like a bomb exploding in my face.”
My boyfriend raised his voice at me for the first time in our friction-free relationship, because I was passionately scrubbing his bathroom at 3 a.m.
A fellow choir member, flabbergasted at what I took to be my brilliant plans to eradicate mental health conditions in the world, shot me a disbelieving look and said, “I’ve never seen you like this.” I wasn’t sure whether he was worried or jealous.
RELATED: Do You Know These Symptoms of Bipolar Mania?
Delusions of Wellness
To me, it just seemed like I had reached a pinnacle in my life after years of chronic depression. I couldn’t wait to thank my psychiatrist for his contribution to my greatness. I wrote him a card saying I had completed my arduous journey to wellness and would no longer be requiring his services.
Instead of clapping and stomping his feet for me, my doctor became more and more appalled as I tried to convince him of my freedom from the frenzy. I, in turn, became furious at the party pooper for raining on my parade.
It wasn’t until he called my sister and begged her to come watch over me that I began to entertain a sliver of doubt.
My sister, a family physician, hopped on the next plane and flew down to Toronto to babysit me and dispense copious amounts of medication and advice. If anyone can convince me of anything, it’s my sister. (She persuaded me that I was adopted when I was 12 — it took my parents months to undo the damage.)
Bit by bit, her certainty that I was experiencing a psychotic episode superseded my insistence that everything was great.
Before 24 hours had passed, I was loaded up on heavy-duty doses of antipsychotics. I actually slept through the night.
By the end of the week, I had come down to earth.
Lack of Insight and 20/20 Hindsight
Looking back on my current (and carefully managed) stability, I’m still blown away by the depths of my denial. After all, I had been exhibiting a textbook case of mania. Why hadn’t I used my medical judgment to uncover my self-evident diagnosis?
I was so certain that I was just happy, at last, and I was furious at those who wanted to pathologize my well-earned contentment.
My sister reminded me of something I already knew: My lack of insight was not my fault; my delusion of wellness was part of the symptom package of mania.
I shudder to think what might have happened if my mania had continued unchecked. My psychiatrist told me I was hours away from requiring urgent hospitalization. I’m lucky that he and my sister prevailed on me to accept that I was unwell instead of special.
I’m also fortunate that my first manic episode led to a diagnosis of bipolar. With my new drug regimen (including a mood stabilizer) and lifestyle changes (regular running, a balanced diet, and mindfulness meditation), I feel a sense of peace I’ve never experienced before. For the first time in my life, I have faith that I will be okay.
UPDATED: Printed as “On My Mind: Queen of Denial,” Summer 2013
June Rawlston is a pseudonym for a Toronto physician who is forging a new career as a writer.
————-
When you’re manic you think you are on top of the world, magnified creativity, and know better than others, rarely listen to logic when it comes to your behavior, quite simply you don’t want the high to end. The truth is it always ends and the higher you go the further you fall. When you fall you may find yourself disoriented, or not knowing where you are, It’s extremely frightening.
Recovering from a manic episode depends on how hard you hit the ground and what happened while you were manic. The recovery time could take months possibly even longer. It’s a long climb up. This is why I keep a close look each day to see if my mood is elevated, it can go from joy to sheer madness very quickly. The key is to track your moods, be aware that your mood is escalating and reach out for help if you continue to escalate.
I spent close to 10 years hypo manic or manic before I fell down the rabbit hole. Crawling out was not pleasant and I spent several weeks in a Psychiatric Hospital to recover.
Stay aware and don’t be tempted by the escalated state, it will bite back.
Melinda
When a Loved One Denies Their Bipolar Diagnosis
Medically Reviewed by Allison Young, MD
Last Updated: 21 Aug 2024
Although it’s incredibly frustrating when someone is in denial of having bipolar disorder, it’s important to remember that acceptance cannot be forced.
It can be upsetting, stressful, and downright incomprehensible when someone with a diagnosis of bipolar disorder denies the mental health condition and refuses treatment. You may find yourself watching helplessly as behaviors tied to untreated bipolar lead to family distress, broken relationships, problems at school and work, money woes, and alcohol and drug abuse.
If you try to help someone in denial, you will probably be accused of interfering if you even mention the word “bipolar.” This is confusing, because it’s very easy for you to see what’s wrong, and naturally you want to point out the problem in hopes that the person will then get help. Often, however, your attempt just makes things worse.
RELATED: 8 Essential Things to Know When First Diagnosed With Bipolar Disorder
It hurts when a person in denial shuts you out, but, sadly, it’s common.
What’s even more confusing is that you can have an honest conversation about bipolar when your loved one is stable, reviving your hopes that the person will enter or stick with treatment. Then … boom! Here comes the denial again.
Learning to Accept That Your Loved One Is in Denial About Their Bipolar Diagnosis
It may be cold comfort to learn that it is very typical behavior for people with bipolar disorder to deny they are “sick” and to avoid treatment, even if they have been in the hospital or taken medications for bipolar in the past.
Also, it’s important to remember that people in denial are usually miserable, in a great deal of internal pain, and can’t see a way out. It’s easy to believe they really can’t see what’s going on. But unless denial is a result of a mood swing — such as strong mania or paranoia — the affected individuals usually know what is happening. They respond to your concern with aggression, because they are trying to protect their decision to deny the brain-based disorder.
It hurts when a person in denial shuts you out, but it’s common. The person prefers to be around others who don’t mention bipolar, and will paint you as the “bad guy” because you are the one who is stating the truth.
RELATED: 10 Ways to Support Someone Who Has Bipolar
There is good news, however. I’ve talked with hundreds of people who moved through denialto eventually admitting that bipolar is at the root of their problems and they needed help. Over and over again, I’ve been told how, despite their relentless inner pain and confusion, they refused help and pushed away the people who cared about them.
It’s when someone realizes they no longer want a life controlled by bipolar disorder that they begin to listen to loving advice instead of fighting back.
Steps to Take When a Loved One Is in Denial About Their Bipolar Diagnosis
If your loved one continues to be in denial of their bipolar diagnosis, here are a few things to keep in mind.
- Find the sweet spot: Are there periods when your loved one is more open to discussion? Oftentimes, people are more receptive during a mild depressive episode. Once you see a pattern in your loved one’s moods, you’ll have a better sense of when to gently start a conversation.
- Set expectations: If a loved one with bipolar is living with you, you have the right to set expectations for behaviors, such as drug use, drinking, yelling, staying in bed all day, staying out all hours, and yes, refusing treatment. You are always in control of what works best for you. It’s not always about the person with the mental health condition. It will be up to you to decide the consequences — and set and reinforce boundaries — if your expectations aren’t met.
- Understand the challenges: Always remember that bipolar is a mental health condition. No one chooses to have bipolar disorder. People in denial can be very unpleasant, and it’s easy to walk away from them, but don’t forget they are suffering. It’s okay to address this directly. Go ahead and say you understand that it must be hard to have someone tell you what to do. Say that you can tell they feel misunderstood. People in denial may get angry or refuse to reply, but they have heard you. Many times, when they get better, they will tell you they heard you.
- Hold onto hope: I’ve known many people who accepted treatment after years of being in denial, often when loved ones learned simple strategies and got them help at the right time. It isn’t easy to hang on until then. Nothing with bipolar disorder is easy! But bipolar is treatable, even for those who currently refuse to admit they are unwell and need help.
UPDATED: Printed as “Fast Talk: The Denial Factor,” Summer 2011
Julie A. Fast is the author of the bestselling mental health books Take Charge of Bipolar Disorder, Loving Someone with Bipolar Disorder: Understanding and Helping Your Partner, Getting It Done When You’re Depressed, OMG, That’s Me! (vol. 2), and The Health Cards Treatment System for Bipolar Disorder. She is a longtime bp Magazine writer and the top blog contributor, with over 5 million blog views. Julie is also a researcher and educator who focuses on bipolar disorder prevention and ways to recognize mood swings from the beginning—before they go too far and take over a person’s life. She works as a parent and partner coach and regularly trains health care professionals, including psychiatric residents, pharmacists, general practitioners, therapists, and social workers, on bipolar disorder and psychotic disorder management. She has a Facebook group for parents, The Stable Table, and for partners, The Stable Bed. Julie is the recipient of the Mental Health America excellence in journalism award and was the original consultant for Claire Danes’s character on the TV show Homeland. Julie had the first bipolar disorder blog and was instrumental in teaching the world about bipolar disorder triggers, the importance of circadian rhythm sleep, and the physical signs of bipolar disorder, such as recognizing mania in the eyes. Julie lives with bipolar disorder, a psychotic disorder, anxiety, and ADD.
Melinda
