One of the most important things a person with Lyme disease needs is clear, concise information.
Here’s a list of useful resources to get you going in the right direction.
LymeDisease.org is one of the foremost Lyme patient advocacy organizations in the United States. We provide a wealth of information on our website–about ticks, Lyme and other tick-borne diseases, prevention, diagnosis and treatment.
Special features include:
Symptom Checklist: Patients can answer a series of questions, print out the filled-in form and take it to their doctor. The printout describes basic facts, explains the two standards of care for Lyme disease, and endorses the ILADS guidelines. It’s a way to help your doctor help you.
Physician Directory: Find a Lyme-literate practitioner near you.
Our blogs keep the Lyme community up to date on news, analysis, and opinion.
Social media. We spread the word via Facebook, Twitter, Instagram and Pinterest.
Our free weekly email newsletters keep you informed on Lyme-related developments. Click here to sign up.
US National Lyme Online Support Group: Information and emotional support for people dealing with Lyme and other tick-borne diseases.
MyLymeData patient registry: This big data research project allows patients to privately pool information about their Lyme disease experiences. So far, more than 17,000 people have enrolled in the project, providing millions of data points on Lyme disease demographics, tick bites, diagnosis, symptoms, lab tests, co-infections, treatment and quality of life. Add your Lyme data to MyLymeData to help find a cure for Lyme disease.
Children and Lyme disease
Basic info about children with Lyme disease
Gestational Lyme disease LymeHope, a Canadian Lyme advocacy organization, has taken a particular interest in the issue of mother-to-fetus Lyme transmission.
LymeAid4Kids–Financial assistance for Lyme treatment for those under age 21.
Lymelight Foundation–financial assistance for Lyme treatment for children and young adults through age 25.
LivLyme Foundation–Financial grants for children with Lyme disease (under 21).
Mothers Against Lyme–Advocacy and education about congenital and childhood Lyme
Video: Lyme Disease & Pregnancy: State of the Science & Opportunities for Research
Book: When Your Child Has Lyme Disease: A Parent’s Survival Guide by Sandra Berenbaum and Dorothy Kupcha Leland.
Book: Brain Inflamed: Uncovering the Hidden Causes of Anxiety, Depression, and other Mood Disorders in Adolescents and Teens by Dr. Kenneth Bock.
Book: Protecting Your Child From the Child Protection System, by Beth Alison Maloney
Book: Finding Resilience: A Teen’s Journey Through Lyme Disease, by Rachel Leland and Dorothy Kupcha Leland.
Article: Healthy Mom Best Prescription for Healthy Baby (The Lyme Times) (PDF)
Wrightslaw.com–Website with information about Special Education law.
PANS/PANDAS
ASPIRE: The Alliance to Solve PANS and Immune Related Encephalopathies
New England PANS/PANDAS Association
Three books by Beth Alison Maloney: Saving Sammy, Childhood Interrupted: The Complete Guide to PANDAS and PANS, and Protecting Your Child from the Child Protection system (The author of these books is the mother of a child who healed from PANDAS. She is an attorney/advocate for the recognition and treatment of PANS/PANDAS, and advises parents about legal issues related to PANS/PANDAS and other complex medical conditions.)
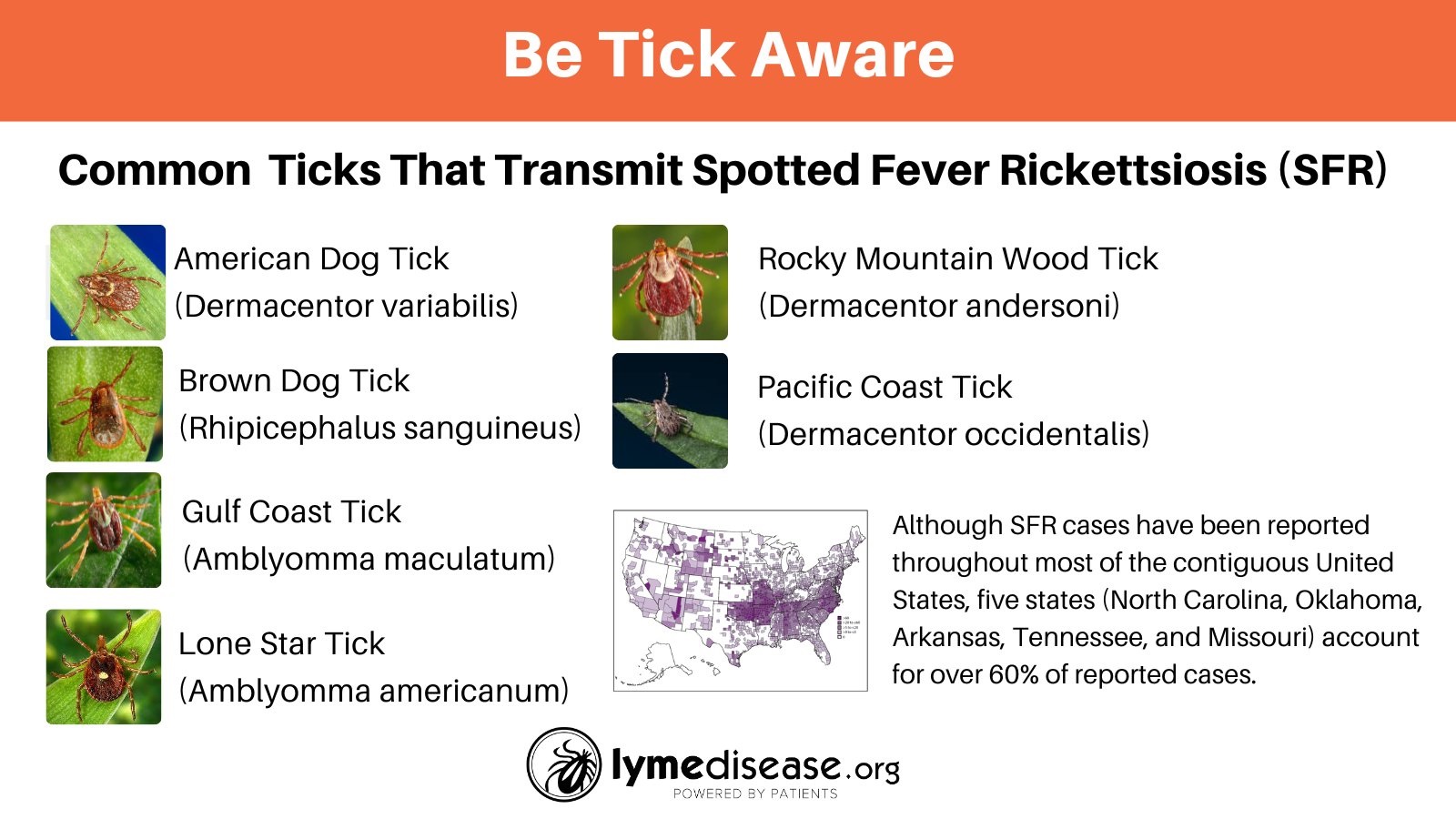
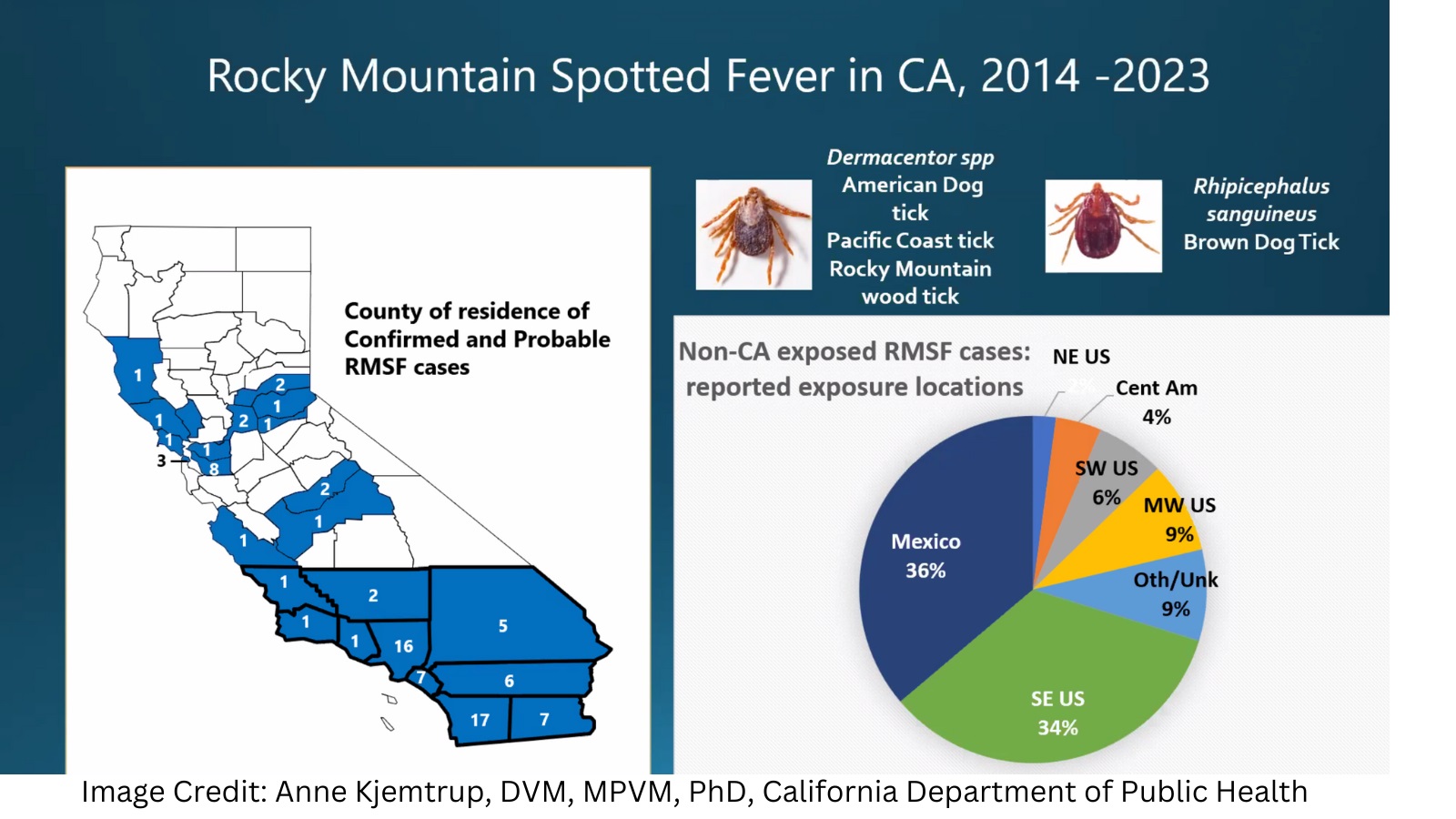
Ticks
How to protect yourself from ticks
Find the repellent that’s right for you (EPA website)
Help! I’ve gotten a tick bite. Now what?
TickEncounter Resource Center—University of Rhode Island
Tick testing. There are various places to get ticks tested. Here are several: IGeneX, TickCheck, Ticknology, Tick Report
MilTICK—free tick testing and identification service available for ticks removed from Department of Defense (DoD) personnel and their dependents.
Mast cell activation syndrome and food-related issues
MCAS, when your immune system goes haywire
The agony of mast cell activation syndrome (MCAS)
Healing from mast cell activation syndrome
What to eat when you’re allergic to everything?
Severe weather can worsen mast cell activation syndrome
Alpha-gal syndrome
There is growing evidence that certain types of tick bites can trigger alpha-gal syndrome (AGS) a life-threatening allergy to red meat and meat-related products.
Alpha-gal syndrome–symptoms, diagnosis, treatment
Other Lyme-related symptoms & issues
Lyme disease can affect the heart in complicated ways
Lyme disease and cognitive impairments
Gastrointestinal manifestations of Lyme
Psychiatric manifestations of Lyme
Medical marijuana and Lyme disease
The dreaded Jarisch-Herxheimer reaction
How Lyme disease can affect your vision
12 ways you can help yourself manage chronic pain
Morgellons
The Charles E. Holman Morgellons Disease Foundation
Morgellons: The legitimization of a disease (book review)
Skin Deep: The Battle Over Morgellons (documentary film)
Treating Lyme disease with disulfiram
What is disulfiram and why does it spark excitement in Lyme community?
Treating psychiatric Lyme symptoms with disulfiram
Co-infections
The Lyme Times Special Issue on Co-infections (PDF)
About Lyme disease co-infections
Mold
Dealing with Lyme disease and mold illness at the same time
Mold Testing Guide (How to test your home for mold)
Your guide to mold in your home
Are you unknowingly ingesting toxic mold?
How to donate blood and tissue for Lyme research
Lyme and pets
Basic information about Lyme and pets
Parasite prevalence maps Educational website includes a US map down to the county level, showing where dogs have tested positive for Lyme, anaplasmosis, erhlichiosis and other diseases. Also, information about protecting your pet from tick-borne diseases.
Companion Animal Parasite Council website has comprehensive information about how to protect your pets from ticks and other parasites.
Books (Treatment, healing modalities, family life)
Brain Inflamed: Uncovering the Hidden Causes of Anxiety, Depression, and Other Mood Disorders in Adolescents and Teens, by Dr. Kenneth Bock
CHRONIC: The Hidden Cause of the Autoimmune Pandemic and How to Get Healthy Again, by Dr. Steven Phillips and Dana Parish
Conquering Lyme Disease: Science Bridges the Great Divide, by Brian A. Fallon, MD, and Jennifer Sotsky, MD
The Deep Places: A Memoir of Illness and Discovery, by Ross Douthat. The New York Times columnist delves into his personal years-long battle with chronic Lyme disease.
Finding Resilience: A Teen’s Journey Through Lyme Disease, by Rachel Leland and Dorothy Kupcha Leland. Based on the journal Rachel kept during the worst years of her illness, with additional insights from her mother, Dorothy.
How can I get better? An Action Plan for Treating Resistant Lyme and Chronic Disease, by Dr. Richard Horowitz
The Lyme Diet, by Dr. Nicola McFadzean. What to eat while healing from Lyme.
Recovery from Lyme Disease: The Integrative Medicine Guide to Diagnosing and Treating Tick-Borne Illness, by Dr. Daniel Kinderlehrer.
TOXIC: Heal Your Body from Mold Toxicity, Lyme Disease, Multiple Chemical Sensitivities, and Chronic Environmental Illness, by Dr. Neil Nathan.
When Your Child Has Lyme Disease: A Parent’s Survival Guide by Sandra Berenbaum and Dorothy Kupcha Leland.
Why Can’t I Get Better? Solving the Mystery of Lyme and Chronic Disease, by Dr. Richard Horowitz.
Books (History, Policy, and Science)
Bitten: The Secret History of Lyme Disease and Biological Weapons, by Kris Newby
Cure Unknown: Inside the Lyme Epidemic, by Pamela Weintraub.
Lyme: The First Epidemic of Climate Change, by Mary Beth Pfeiffer.
Film and Video
I’m Not Crazy, I’m sick, Lyme documentary, available on various streaming services.
The Quiet Epidemic, documentary film about chronic Lyme disease, available on various streaming services.
Under Our Skin, award-winning Lyme documentary film.
Under Our Skin 2: Emergence (sequel)
The Red Ring, documentary takes a global look at Lyme disease.
Your Labs Are Normal, feature film based on real-life experiences.
Financial assistance
LymeTAP.com–Lyme Testing Access Program. Financial assistance for Lyme diagnostic testing.
Needymeds.com–Clearing house for information about various kinds of financial assistance for obtaining medication.
Lymelight Foundation–financial assistance for Lyme treatment for children and young adults through age 25.
Lyme Treatment Foundation–financial assistance for Lyme treatment. No age restrictions.
LivLyme Foundation–Financial grants for children with Lyme disease.
LymeAid4Kids—grants for young Lyme patients (up to age 21).
Partner in Lyme—grants for Lyme treatment for residents of Connecticut.
Applying for Social Security benefits for Lyme disease
Outside of the United States
ALCE Asociación de Lyme Crónico España (Spain)
Canadian Lyme Disease Foundation
LymeHope (Canada)
LYRI (Mexico)
Lyme Disease Action (UK)
Lyme Disease Association of Australia
Karl McManus Foundation (Australia)
Association Luxembourgeoise Borréliose de Lyme (Luxembourg)
Onlyme-aktion.org (Germany)
Lymevereniging (Netherlands)
TOUCHED BY LYME is written by Dorothy Kupcha Leland, LymeDisease.org’s Vice-president and Director of Communications. She is co-author of When Your Child Has Lyme Disease: A Parent’s Survival Guide. Contact her at dleland@lymedisease.org .
Melinda