Pain Week is a publication specifically for Pain Doctors, one I haven’t heard of before. This mini article and Podcast shine a light on a topic those who suffer from chronic pain already know. Pain medication is not being prescribed when needed and specialized pain care is dwelling.
This Podcast is very interesting, we now know why most doctors are running for the hills, as they say.
Melinda
A SINGLE POINT OF ACCESS FOR FRONTLINE PRACTITIONERS
Aug 10, 2020
At the 2018 Department of Justice (DOJ) Opioid Summit, then-Attorney General Jeff Sessions remarked that opioid prescribing had reached its lowest point in 18 years. Still, the DOJ is committed to reducing opioid analgesic prescriptions an additional 30% to 33% within the next 3 years. More than ever, prescribers of controlled prescription medications are under intense scrutiny from lawmakers, regulators, and payers. At the same time, some 50 million adults in the US have persistent pain, nearly 20 million of whom experience pain that interferes with daily life or work activities.
As noted by the Pain Management Best Practices Inter-Agency Task Force (PMTF) in its December 2018 draft report, the trend of healthcare professionals opting out of treating pain has exacerbated the shortage of pain management specialists, leaving some patients without access to individualized care. In this session, a partner in a Washington, DC based health law firm will discuss recent legislative and regulatory activity at the federal level and trends in criminal enforcement. He will also discuss noteworthy developments at the state level and analyze the anticipated benefits, drawbacks, and unintended consequences of such actions on people with pain and those who treat them.
Topics will include the implications of recently passed comprehensive opioid legislation—the SUPPORT for Patients and Communities Act; a draft report on pain management best practices by PMTF and the pushback against it; and efforts to reform the federal approach to investigating controlled-medication prescribers.
Written by Dr. Eric Perry Image Credit: Pixabay “A friend is a gift you give yourself.” ~Robert Louis Stevenson What kind of friend are you? Are you attentive, kind and compassionate or, are you neglectful, uncaring and critical? Scrolling through quotes on the internet, I was reminded of the immense value we place on friendship. […]
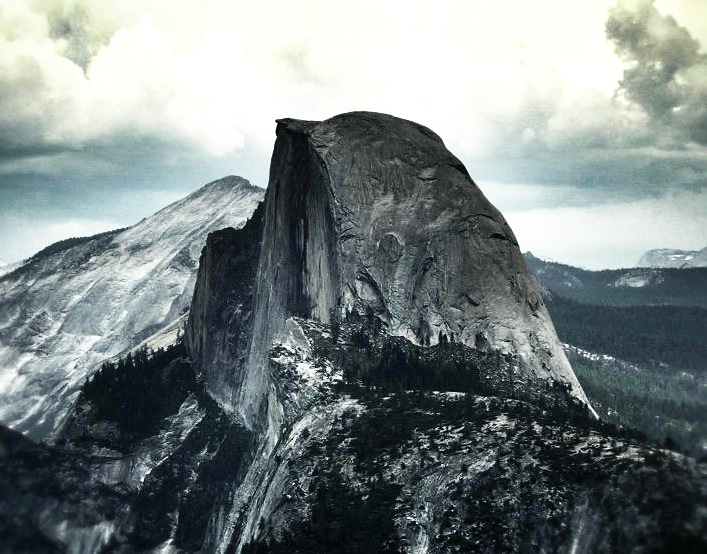
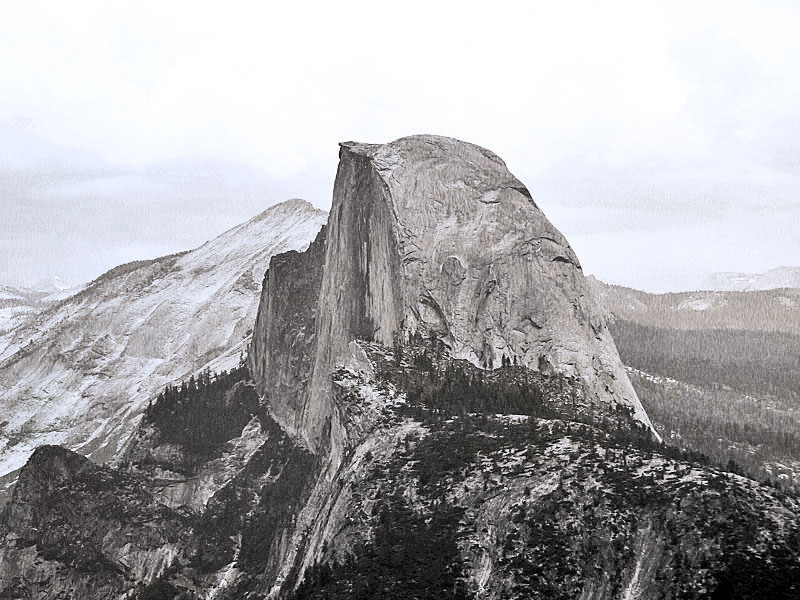
I hope you enjoy the different renditions of Half Dome at Yosemite National Park, California in America. If you have not been, please consider going, or put on a bucket list. The park is a World Wonder! Thank you for stopping by today, I truly appreciate you and so glad to see you.
Which photo is your favorite? The first one reminds my of The Wild West, the old movies I watched with gramps growing up. I went for a slightly different effect with each one, not that any are masterpieces, remember I’m an amatuer photographer. I look forward to hearing your replies.
Self-care may seem like a luxury but in fact, it’s important for everyone to take time out for self-care. Self-care or taking a few minutes for ourselves is critical to our mental health. Our mind and body need a break, a chance to unwind, to refocus and there are many ways to unwind.
I do many things for self-care depending on how much time I have. If I have 30 minutes I may take a hot aromatherapy bath, give myself a manicure, if I’m crunched for time a hot foot soak is very relaxing. Simple ways are enjoying a candle for a few minutes, meditating, watching the birds, or just taking a walk around my backyard to clear my head.
Men need self-care just as much as women, the manner in which you find a moment of joy may look different. A good foot soak is always a great way to relax, meditation, taking a 15-minute power nap, hot shave, scalp massage, hot bath, or even stretching exercises and aromatherapy is can be relaxing.
Does it seem like you can’t complete even the simplest task without being distracted? Texts, emails, social media alerts, noisy colleagues, ringing phones… Friends, you are not alone.
Distracted thinking — aka daydreaming or mind-wandering — affects everyone. In fact, researchers have found that people think about something other than what they’re actually doing — or supposed to be doing — almost half of the time. Turns out that a wandering, easily distracted mind is actually the default mode for the human brain.
Succumbing to distraction over and over, though, can build stress, foster unhappiness, and even lead to depression. So if you’re one of the many looking to figure out how to handle distractions and improve your ability to focus, take comfort in the fact that research has shown a way forward.
One word: mindfulness.
Mindfulness means maintaining moment-to-moment awareness of where you are and what you’re doing. At work, for instance, it means you’re focused on the project in front of you; walking with a friend, it gives you the ability to really focus on your surroundings and your conversation. Scientists have shown that you can actually train your brain to become more mindful. Like anything else, it just takes practice.
Ready to get started? These three practices have all proven useful in building mindfulness.
1. Mindfulness-based stress reduction (MBSR)
MBSR training has become a recognized way to help people learn to avoid distractions and increase their attention to the task in front of them. It can also help improve memory, motivation, and autonomy — all things likely to make you (and your boss) happier. MBSR programs typically include breathing, stretching, and awareness exercises.
2. Meditation
Meditation aims to increase your awareness of the present moment and help you develop a gentle, accepting attitude toward yourself. Regular meditation practice has been shown to actually alter the brain — in a good way. One study showed that the area of the brain dedicated to regulating your emotions was significantly larger in meditators. In other words, in a world determined to trip you up with distractions and unpleasant surprises, meditation can help you stay more positive and more focused.
3. Mindful movement
The hallmarks of mindful movement, or yoga — structured breathing, controlled movement, mental focus — make it sound like the perfect antidote to stress and distracted thinking, but does science back that up? Yes, over and over again. Many studies have found that, after beginning a yoga program, people feel less stressed, more focused, even more optimistic. In fact, yoga’s been found to be even more beneficial to people who’re highly stressed.
In today’s so-called attention economy, the world is actually being designed to distract you. Everybody wants your attention, and they want it right now. But you can take back control of your focus, shed that stress, and wake up happier to meet your day.
Ready to commit to becoming more mindful? Great, go for it!
Life can be stressful and times like these are not making it any easier. That is why spending time outside is encouraged for your mental health. Research has shown that time outdoors gardening can lift your spirits. Playing in the dirt can reconnect you with nature, allowing you to see the bigger picture and giving you a different perspective. Here are some surprising ways gardening can do wonders for your mental health.
Sometimes things are just the way they are and there may not be much you can do about it. In times like these, practicing acceptance comes in handy to keep your mental health in check. Life is unpredictable. Gardening will help you realize that life will blossom in the way it wants. Of course, you can provide an ideal environment for your plants to be strong, healthy and nutritious, but after a while, you have to let it do its own thing.
Allows You To Let Go Of The Need For Perfection
Life is not perfect. Nothing is perfect. Desperately trying to make things perfect will run you ragged and leave you frustrated. Wanting perfection can cause you to miss opportunities, damage your relationships, and can even paralyze you from trying something new. Nothing will teach you that more than planting your favorite vegetable or fruit. No matter how carefully you try to map out how your garden will look, how it will grow, or how many Ryobi trimmer reviews you read, there are many factors that cause imperfections in your garden. These are things like insects, diseases of your plants, bad weather, and pests. Gardening will force you to relinquish the need for perfection.
Allows You Change Your Mindset
One of the ways to maintain your mental health is to change your mindset from a fixed mindset to a growth mindset. When you have a growth mindset you believe that you are constantly learning even when things do not go as planned. You look at those situations as an opportunity to learn and grow instead of failure. It can change your perception of making mistakes. Gardening can help you work on building up that mindset. You cannot fail at gardening, even if all your plants die. All that you did is learn how to better take care of your plants for the next time.
Allows You To Connect
Gardening allows you to connect with people and the world. For one, gardening is a hobby enjoyed by many people around the world. If you garden, you will likely find a friend who enjoys gardening too. It also allows you to connect with the earth. Think about it; you are playing in its dirt all day and you are adding to it. You are creating an impact. Gardening almost feels like being a parent because you develop a bond with the plot of land you are tending as well as the plants that sprout out of it.
This post is from 2016 and on a topic I feel is important to discuss. When you take addictive medication, it’s essential to take the prescribed dosage. I was also suffering terribly from Lyme Disease at the time. You can see how out of control my life became by self-medicating and not taking the prescribed dosage.
Xanax is an anchor drug in my medication combo for treating Anxiety/Bipolar Disorder. I’ve taken Xanax for 15 years, it works miracles in keeping me grounded. Working quickly is an advantage with little to no side effects, EXCEPT ADDICTION. The downside side is addiction happens quickly after starting. For me withdrawal starts on the second day, my fourth day I look like a street addict who would sell my soul for a pill.
The emotional and physical breakdown took me to hell. My deep secrets/scars laughed and taunted me.
Here are some of the delusions I experienced.
Learned a new language
Surviving in the desert-like Jesus
Discovered potential link for Postpartum Depression
In touch with my families Indian blood
Could feel natural body rhythm
Felt small earthquake
Saw Bobcat tracks on the front tree
Started writing Country songs
Tweeting Gwen Stefani, Blake Shelton, and Pharrell, talked to Gwen and Blake several times, Pharrell retweeted twice. I was flooded with people wanting to follow me after seeing tweets from Gwen. I was overwhelmed.
Locked all computers down, trying to keep me from writing.
The physical pain is unbearable
Anger, pain, begging God to stop kicking me in the stomach, wailing, screaming, throwing up, four days without food.
Having to transition back one medication a day at a time
Delayed Lyme protocol by a week, reschedule the trip to DC by a month
More damage to areas already injured
Strain on marriage
Xanax is a standard drug and withdrawal doesn’t cross my mind. I kept some pills in my purse, pills in my office, and the remaining pills went into master pill caddy. The trouble is not keeping up with how many total pills you’ve taken. I take several addictive medications for my mental illness and 4-5 addictive medications for Lyme treatment.
I am in pain 24/7 and resist taking pain medication instead I try to cover the pain with Xanax. I take two Xanax and I’m asleep a good 4-6 hours without pain. The Lyme Protocol calls for 4-5 addictive medications but they rarely put me to sleep. It worked the opposite and I would stay awake 2-3 days at a time which made my pain even worse.
Now all medications stay in the bottle or main pill cases.
I wrote most of this during or right after my withdrawal, you can see how my mind was not in control. Not only was my mental illness not under control but my physical health was badly damaged. Please keep all of your medication is one place and make sure you’re taking the prescribed dosage.
I am reblogging this post because I’m having to go thru withdrawal from Percocet & Belbuca since my Pain Management doctor fired me. I was scared to go to the office because of Covid and he didn’t offer Telehealth. The front desk kept insisting I had to come in, that he would not make any exceptions. So he fired me. He only wrote two weeks’ worth of medication and offered no referral. I can’t find and get into seeing another Pain Management doctor within two weeks. I asked for a month and was told NO. Belbuca is so expensive my pharmacy would not fill for just two weeks, they couldn’t have two weeks worth of an expensive drug setting on their shelves. I’ve since found out that Texas State Law required doctors who managed patients with chronic health conditions to offer Telehealth appointments thru September 1, 2020. I have filed a complaint with the Texas Medical Review Board.
Please remember to have a backup doctor should this happen to you. I did get a referral from my knee surgeon but I’m in no hurry to go in with Covid still on the rise in my area. I’ll deal with the withdrawal, just suck it up and wait. Covid is much worse!
As many fo you know I am not able to participate in awards at this time due to my health however I do want to bring attention to the gut-wrenching blog A Prisoner By No Crime of My Own.
Jodie shares her journey of death and abuse with a no hold bars approach and draws parallels to the Bible along the way.
Please check out her blog, you will not be sorry and I’m sure you will follow her.
I found his cell phone in the ashtray along with ten pairs of fingernail clippers, a knife, a small pair of scissors, a Corona Light bottle top, and three nickles and nine pennies.
On top is my favorite knife, the camping type with a fork and spoon, he gave to me when I was little, and a paper-towel covers them all, it’s been there for over eight years untouched.
The ashtray sat by my grandparent’s telephone for as long as I can remember. They didn’t believe in buying something new unless it was broken or you could no longer use it. The ashtray was very useful.
When I removed the paper towel today, the memories of my gramps came flooding back like a wave.
“If you’re going to be late to work, don’t go in.”
“If you can get out of bed, you can go to work”
“If you borrow something, give it back in better shape than when you borrowed it.”
He also taught me to drive. I was fourteen, we went to the river bottoms, two metal trashcans in the back of the 1969 Ambassador. He set them apart the right distance and had me practice until nightfall. I was still knocking down cans when we left. I did pass my driver’s test though.
One of the hardest memories was weeks before his death, telling him to call friends and family to let them know he was dying. Sitting in front of him, I dialed the numbers, handing him the phone and listened as he cried telling people he was no longer going to be here. It was one of the most difficult days of my life.
My gramps was the greatest man I’ve ever known, a true gentleman, a stand-up guy, God broke the mold when he made my gramps.
Today we celebrate the end of the conflict with Japan which brought to an end the Second World War.
Let’s not forgot those who made the ultimate sacrifice and who stayed behind to support the war effort. My gramps was on the front lines in Germany and my granny was a Rosie the Riveter, I’m so proud to know my grandparents fought for my freedom and the freedom of others. Their efforts help shape the world as we know it.
Happy Friday! I am so glad you stopped by today. Have a great weekend and please wear a mask, I want to see you healthy! I really like this quote, we can do many little things to give to people and no amount of stuff will ever feel as good. :)
Stress plays a very important role in our mental health, good stress, and bad stress. Good stress motivates us to move forward, reach new limits, and push us to the next level. Bad stress on the other hand is detrimental to our overall well being and can cause hair loss among other ailments.
Telogen effluvium. In telogen effluvium (TEL-o-jun uh-FLOO-vee-um), significant stress pushes large numbers of hair follicles into a resting phase. Within a few months, affected hairs might fall out suddenly when simply combing or washing your hair.
Trichotillomania. Trichotillomania (trik-o-til-o-MAY-nee-uh) is an irresistible urge to pull out hair from your scalp, eyebrows or other areas of your body. Hair pulling can be a way of dealing with negative or uncomfortable feelings, such as stress, tension, loneliness, boredom or frustration.
Alopecia areata. A variety of factors are thought to cause alopecia areata (al-o-PEE-she-uh ar-e-A-tuh), possibly including severe stress. With alopecia areata, the body’s immune system attacks the hair follicles — causing hair loss.
Stress and hair loss don’t have to be permanent. If you get your stress under control, your hair might grow back.
If you notice sudden or patchy hair loss or more than usual hair loss when combing or washing your hair, talk to your doctor. Sudden hair loss can signal an underlying medical condition that requires treatment. If needed, your doctor might also suggest treatment options for your hair loss.
Happy Wednesday Friends! So glad you stopped by today I appreciate you. It’s August in Texas, the hottest month of the year and thermometer is over 100 degrees. I’m thrilled to have flowers alive in August, it’s taken lots of hot nights watering them to keep them alive.
This is supposed to be Wordless Wednesday and I said a lot. Have an awesome day!
As many of you know I can’t participate in awards any longer due to my health however, I do want to call attention to the person and the great blog who nominated me.
She’s an ex mental health nurse who has experienced mental illness first hand. Caz is dedicated and passionate about raising awareness and fighting the stigma around mental health.
I love this quote on her site, it’s the simple things we can all do each day that makes a big difference.
“None of us, including me, ever do great things. But we can all do small things, with great love, and together we can do something wonderful.” – Mother Teresa
Please check out her blog and follow her, she has an extensive archive on a wide range of mental health topics and is a great resource for all topics on mental illness.
This article is great news for those who are leary of using DEET to prevent tick bites. Hopefully, it will be on the market soon. I’m all for using natural products when I can.
An undated photo provided by the Centers for Disease Control and Prevention shows an Asian longhorned tick. The Environmental Protection Agency has approved nootkatone, which repels ticks, mosquitoes and other dangerous bugs for hours, but is safe enough to eat. (James Gathany/Centers for Disease Control and Prevention via The New York Times)
Adding a new weapon to the fight against insect-borne illnesses including Lyme disease and malaria, the Environmental Protection Agency on Monday approved a new chemical that both repels and kills ticks and mosquitoes.
The chemical, nootkatone, an oil found in cedar trees and grapefruits, is so safe that it is used by the food and perfume industries.
Nootkatone is considered nontoxic to humans and other mammals, birds, fish and bees, the EPA said in a statement.
Diseases caused by the bites of ticks, mosquitoes and fleas have tripled in the United States in the last 15 years, the Centers for Disease Control and Prevention said in a 2018 report. They include Lyme disease, anaplasmosis and Rocky Mountain spotted fever from ticks; West Nile, dengue, Zika and chikungunya from mosquitoes; and plague from fleas.
In tropical countries, malaria and yellow fever are major killers, and elephantiasis is also spread by mosquitoes. Lethal Crimean-Congo hemorrhagic fever is spread by ticks, and kala azar is spread by sandflies.
Manuel F. Lluberas, a public health entomologist who has worked on mosquito-control campaigns around the world, said that he hoped that nootkatone would be accepted by people who fear synthetic repellents and that it could be made cheaply enough to be bought by foreign aid programs like the President’s Malaria Initiative.
The EPA registration applies only to nootkatone as an active ingredient, the statement said. Any formulations using it in the future will have to be tested and registered separately.
The chemical repels mosquitoes, ticks, bedbugs and fleas — and, in high concentrations, kills them, according to the CDC. It may also be effective against lice, sandflies, midges and other pests, some of which can carry lethal diseases.
It is not oily, lasts for hours and has a pleasant, grapefruitlike scent, said Ben Beard, deputy director of the division of vector-borne diseases at the CDC, naming two grapefruit-flavored sodas.
“If you drink Fresca or Squirt, you’ve drunk nootkatone,” Beard said.
Nootkatone works differently from previous classes of insecticides and can kill bugs that are resistant to DDT, pyrethroids and other common insecticides.
Experts in insect-borne diseases greeted the news with cautious enthusiasm.
“Its use as an insecticidal soap has great potential,” said Duane J. Gubler, a former CDC chief of vector-borne diseases.
One proposed use is in soaps that people in tick-infested areas could shower with, repelling and possibly killing ticks that try to attach to them.
Joel R. Coats, a specialist in insect toxicology at Iowa State University, said his lab had tested nootkatone and found it to be “an impressive repellent but a weak insecticide.”
It repels ticks even better than synthetics like DEET, picaridin or IR3535 do, Coats said, and it is their equal at repelling mosquitoes.
Unlike citronella, peppermint oil, lemon grass oil and other repellents based on plant oils, he added, nootkatone does not lose its potency after about an hour but lasts as long as the synthetics.
Although it can also kill insects, he said, doing that takes so much of the chemical that it may not be practical.
“Most plant terpenes will kill bugs if you go to a high enough dose, but I haven’t seen any data that supports using it as an insecticide,” Coats said, using a term for aromatic oils exuded by many plants to repel invasive insects. “I’ve seen lots of data on it as a repellent.”
Mikkel Vestergaard-Frandsen, owner of the Vestergaard company, which makes insecticide-impregnated nets to fight malaria, said he was interested in the compound but wanted to know more about it.
Because babies sleep under the nets, any insecticide in them must be safe.
In many areas, mosquitoes have developed resistance to the pyrethin-based insecticides now used in nets, which are synthetic versions of a chemical found in chrysanthemum flowers.
A version of nootkatone that can linger in netting fabric for years would have to be developed, but good repellents usually dissolve too quickly for that, he said.
The CDC discovered nootkatone’s repellent properties almost 25 years ago as part of a search for new tick-control compounds to fight Lyme disease, Beard said.
They investigated cedar bark and chips “because there are all these folk tales that cedar repels insects — and people keep their clothes in cedar chests,” he said.
Cedar wood itself had very little effect on ticks, he said, but Oregon State University scientists working with the agency found the terpene oil of the Alaskan yellow cedar to be powerfully repellent. The Latin name of the tree is Cupressus nootkatensis, which comes from the Nuu-Chah-Nulth people of Canada.
It is “not known in great detail” how nootkatone works, Beard said, but it appears to activate octopamine receptors, which in insects send electrical impulses from one nerve cell to the next. Unable to turn off the signal, the bugs twitch to death.
In mammals, adrenaline — which is chemically related to octopamine — performs the same function. But the compound does not trigger adrenaline receptors.
Later the agency realized that the same chemical, originally derived from grapefruit rinds, was used as a flavoring and in perfumes.
The CDC licensed its patent to a Swiss company, Evolva, which isolates the chemical from fermenting yeast.
But doing the safety studies required for EPA registration was too expensive until the 2015-16 Zika epidemic came along, Beard said.
That epidemic prodded Congress to appropriate money for mosquito control, and the CDC transferred some of it to BARDA, the Biomedical Advanced Research and Development Authority, which contracted with Evolva to finish the research.
Zika funding “was the key to moving the boulder up the hill,” Beard said. But because nootkatone works well on both mosquitoes and ticks, he added, “it wasn’t a bait-and-switch.”
Yoga students may present with a variety of physical health concerns, such as chronic pain or injury. As a yoga instructor, it is important to become familiar with student histories so that the teacher can ensure the yoga studio remains a safe space for students. Overall, engagement in yoga practice has been consistently increasing in […]
The CDC decries abrupt, involuntary dose reductions and patient abandonment without acknowledging its responsibility for those unintended but foreseeable consequences.
Deborah Dowell (CDC)
In a New England Journal of Medicinecommentary published today, the authors of the opioid prescribing guidelines that the U.S. Centers for Disease Control and Prevention issued in 2016 reiterate the agency’s recent warning that it does not recommend abrupt or nonconsensual tapering for patients who are already taking high doses of narcotic analgesics for chronic pain. “Unfortunately, some policies and practices purportedly derived from the guideline have in fact been inconsistent with, and often go beyond, its recommendations,” write Deborah Dowell, Tamara Haegerich, and Roger Chou. Those policies and practices, they say, include “inflexible application of recommended dosage and duration thresholds and policies that encourage hard limits and abrupt tapering of drug dosages, resulting in sudden opioid discontinuation or dismissal of patients from a physician’s practice.”
Dowell, Haegerich, and Chou warn that patients forced to reduce their doses “could face risks related to withdrawal symptoms, increased pain, or unrecognized opioid use disorder” and “if their dosages are abruptly tapered may seek other sources of opioids or have adverse psychological and physical outcomes.” They also worry that doctors are responding to the CDC’s advice about the potential risks of opioids by “dismiss[ing] patients from care” or declining to prescribe opioids at all, “even in situations in which the benefits might outweigh the risks.” Dowell et al. say “such actions disregard messages emphasized in the guideline that clinicians should not dismiss patients from care, which can adversely affect patient safety, could represent patient abandonment, and can result in missed opportunities to provide potentially lifesaving information and treatment.” And they note that the guidelines have been improperly applied to “patients with pain associated with cancer, surgical procedures, or acute sickle cell crises.”
The CDC’s recognition that misinterpretation of its guidelines has resulted in needless suffering, patient abandonment, and “adverse psychological and physical outcomes” (including suicide) is welcome, if overdue. “This article should allay anxiety among physicians who prescribe responsibly for patients with chronic pain,” says Sally Satel, a Washington, D.C., psychiatrist who helped organize a March 6 letter to the CDC in which hundreds of health professionals and addiction specialists, including three former drug czars, expressed concern about the unintended consequences of the CDC’s advice. “No longer can any clinician, insurer, health care system, or pharmacist claim ‘the CDC Guideline says’ when it comes to tapering or discontinuation.”
Stefan Kertesz, a University of Alabama at Birmingham pain and addiction specialist who worked with Satel on the letter to the CDC, was also heartened by the NEJM article. “We needed CDC and its guideline’s authors to do precisely what they have done, which was to speak with vigor and clarity to the pressing ethical concern we laid out in our letter,” he says. “In affirming that the guideline did not call for hard dose cutoffs and forced tapers, the guideline’s authors have effectively called for recalibration of policies by insurers, by Medicaid authorities, and by agencies that have set ‘the number of patients above a given dose’ as the primary indicator of bad care.”
The letter to the CDC included testimony from hundreds of patients who have suffered the consequences of that ham-handed approach. “The trauma to patients who have been living in terror these past three years nearly broke my heart many times,” Kertesz says. “The only possible step has been for people familiar with the nexus of science and health policy to speak openly about the problems we have seen, and to trust that most people ultimately want to do what’s right.”
Yet Dowell et al. conspicuously fail to take any responsibility for the unintended but foreseeable harm caused by their advice. When a document is as widely misconstrued as the CDC’s guidelines have been—by insurers, regulators, legislators, pharmacists, and law enforcement agencies as well as clinicians—it is fair to ask how the authors left themselves open to misinterpretation.
According to the guidelines, “Clinicians should use caution when prescribing opioids at any dosage, should carefully reassess evidence of individual benefits and risks when considering increasing dosage to ≥50 morphine milligram equivalents (MME)/day, and should avoid increasing dosage to ≥90 MME/day or carefully justify a decision to titrate dosage to ≥90 MME/day.” The implication is that doses of 90 MME or more per day are rarely, if ever, medically justified.
It is hardly a stretch for physicians with patients who exceed this arbitrary threshold, including patients who have been functioning well on high doses for years, to worry that they will be perceived as practicing outside the bounds of proper medical care. Given the scrutiny that regulators and law enforcement agencies such as the Drug Enforcement Administration (DEA) have been applying to doctors in response to the “opioid epidemic,” prescribing practices portrayed as extreme and dubious by the CDC are apt to attract unwelcome attention that could jeopardize a physician’s livelihood and liberty.
“We still, unfortunately, have physicians who worry about capriciousness on the part of the DEA,” Satel notes. “That is the next step in efforts to ensure that doctors can continue to serve pain patients who have been benefiting from opioids.” While “the DEA does indeed have a job to do,” she says, “doctors are confused about what could make them a target.”
How doctors respond to anti-opioid pressure will depend on how they weigh their duty to patients against their personal risk. In this context, forced tapering and abandonment were predictable outcomes, even though the CDC guidelines say doctors should reduce doses only when the risks outweigh the benefits and describe the process as collaborative and consensual.
“Clinicians should empathically [sic] review benefits and risks of continued high-dosage opioid therapy and should offer to work with the patient to taper opioids to safer dosages,” the guidelines say. “For patients who agree to taper opioids to lower dosages, clinicians should collaborate with the patient on a tapering plan.”
Dowell et al. complain that “the guideline has been misimplemented,” saying “policies invoking the opioid-prescribing guideline that do not actually reflect its content and nuances can be used to justify actions contrary to the guideline’s intent.” But those nuances were bound to be lost amid the fear and anxiety caused by the government’s crackdown on prescription pain relievers.
Notwithstanding Dowell et al.’s disavowal of “hard limits and abrupt tapering,” that is what happenedacross the country after the CDC guidelines came out, as reflected in this sign at a doctor’s office in Washington state. “Beginning February 2017,” it says, “Morphine Equivalency Dosing WILL decrease until CDC guidelines are met by June 2017. Target is 90mg of Morphine equivalency per day, or less. All medication adjustments will be based on this new clinic policy.”
While decrying involuntary and precipitous tapering, Dowell et al. present the general decline in opioid prescribing as a sign of progress. “Although outpatient opioid prescribing had been declining since 2012,” they write, “accelerated decreases—including in high-risk prescribing—followed the guideline’s release.” Yet the continuing drive to reduce the volume of opioids prescribed in the United States has encouraged doctors, insurers, and policy makers to target patients on high doses, who consume a disproportionate share of the total. Kertesz emphasized that point at a recent conference in Charleston.
Dowell et al. do not acknowledge the downside to the decline in opioid prescribing, which has been accompanied by a surge in opioid-related deaths as both patients and nonmedical users turn to the black market, where the drugs are much more dangerous because potency is highly variable and unpredictable. Nor do they question their emphasis on the 90-MME threshold, which is scientifically problematic for several reasons. It assumes that analgesic effect corresponds to overdose risk and that different opioids can be reliably compared to each other based on fixed ratios. It ignores numerous factors that affect how a patient responds to a given dose of a particular opioid, including obvious considerations such as the patient’s weight, treatment history, and pain intensity as well as subtler ones such as interactions with other drugs (which can suppress or amplify an opioid’s effects) and genetically determined differences in enzyme production and opioid receptors.
“Policies should allow clinicians to account for each patient’s unique circumstances in making clinical decisions,” Dowell et al. write. The CDC’s 90-MME threshold, however it was intended, has in practice encouraged a much less discriminating approach, one that sacrifices patients’ welfare for the sake of conforming with the perceived demands of the federal government.
“The CDC bears full responsibility for how these arbitrary dose levels are being implemented throughout the country and the consequences for the people in pain,” Lynn Webster, a former president of the American Academy of Pain Medicine who signed the March 6 letter to the CDC, told me last year. “I said at the time when they were proposed that if something comes from the CDC as a guideline, it is more than a guideline. It will be interpreted basically as a level of dosing that if you exceed [it], then you are at legal jeopardy.”
Dorothée Lorang, a filmmaker who lives in Nantes, France, has two children. One of them, Axel, is the central character in a remarkable video called “Axel and the True Story of an Imaginary Illness.”
Can you guess what the “imaginary illness” is?
Though under an hour long, the story of Axel and his family packs quite an emotional wallop–along with a lot of critically important information. It is both poignant and illuminating.
We learn about the difficulties of getting properly diagnosed and treated for Lyme disease in France, the pain and frustration of a suffering family, and the indomitable spirit of a little boy who’d rather pretend he’s Batman than undergo pushing and prodding from medical doctors who ultimately don’t believe he’s really sick anyway. (Who can blame him?)
Other issues that play a part: a mother and father’s dogged search for answers when they keep running into brick walls; the question of gestational Lyme disease; the effectiveness of antibiotic vs. alternative therapies; and the importance of Lyme patient activism.
This extraordinary film shares its story in a disarmingly simple way. (When in fact, we all know that Lyme disease can devastate a family in the non-simple manner of a runaway train plunging into a ravine, yes?)
“Axel and the True Story of an Imaginary Illness” doesn’t dispute the complexities involved. Yet, it offers a calm clarity as the parents discover new treatment approaches and weigh the decisions they must make to help their son.
The film is in French, with English subtitles. It’s available on Vimeo, where you can watch a snippet of it for free. Watching the whole thing will cost you $2.83. I found it well worth the price of admission.
(If you decide to rent the film, make sure to click the “CC” button in the lower right-hand corner of the frame. That turns on the English subtitles. I confess, it took me a while to figure that out.)
For many people around the world, it’s still hot outside and you’re enjoying outdoor activities. I am reposting this as a reminder of how serious Lyme Disease is, it will change your life forever if not diagnosed in the first 2-4 weeks. Around 30% of people do not get the bullseye rash and you have no way to know you have been bitten by a tick. We are talking about ticks smaller than a grain of rice! Think about how hard they are to find in your hair. I’ve been ill since 2012 and was diagnosed shortly after as having Lyme disease, it’s been a long hard road.
I’ve recently been diagnosed with Hypogammaglobulinemia which is an autoimmune disorder of the blood. If severe enough Plasma Infusion Therapy is required.
Here’s what Wiki had to say:
Hypogammaglobulinemia is a problem with the immune system in which not enough gamma globulins are produced in the blood (thus hypo- + gamma + globulin + -emia). This results in a lower antibody count, which impairs the immune system, increasing risk of infection.
I’ve never wanted a blood transfusion in the past and lucky one was never required. I don’t know how I feel about plasma, there isn’t really an option. Your body must have white blood cells to fight off every type of infection including the common cold.
I saw a Hematologist who thankfully told me I don’t have bone marrow cancer and referred me to an Immunologist. I had a Telehealth appointment with the Immunologist only to find out he no longer does Infusion Therapy and has to refer me to another Immunologist. Be sure you ask if the Immunologist you’re referred to does the Infusion Therapy before your appointment in case it’s needed.
He went ahead and ordered blood work for which I had to go to the lab during this crazy time. A lab with sick people is the last place I wanted to be. They were working by appointment and only allowing four people in the waiting room which made me feel better.
The feeling of comfort went away when the person in front of me didn’t have on a mask and was not offered one, worst the lady behind the desk was wearing her mask on her chin and coughed. What the Hell! Now two weeks later I find out my lab work is lost.
Next week I start over. It’s calling the doctor’s office, asking for the referral, and letting them know there isn’t a need for blood work since he doesn’t provide the needed therapy.
Can I say for sure this new autoimmune disorder is tied to Lyme? No, but I can’t forget the words of my doctor when I was first diagnosed, Lyme will cause other autoimmune disorders and illnesses. My change is health is proof of what he said is true.
PLEASE take Lyme Diseases serious. I can’t stress enough how important prevention is, use 20% DEET in your spray or sunscreen, and checking for ticks is a critical part of prevention.
Melinda
Update February 27, 2020
Warm weather is right around the corner, I know some of us are experiencing freezing weather but Spring is around the corner. The south will start to feel great outdoor weather in a matter of weeks. Lyme has left made my life hell, I don’t want you or anyone you love to go thru the same painful illness.
Please remember!!!!! There is no cure for Lyme and the diseases you get from your immune system being compromised can be life-threatening. As you go for the first hike, long walk with the dog, picnic with the kids, make sure you prepare for ticks. You don’t have to see cows or be anywhere near cows. A silly notion. The only sure way to prevent the ticks don’t stick to you is 20% DEET.
I didn’t want to use DEET in the past, and that was just to ward off flying bugs. DEET is the only recommenced prevention for tick-borne illnesses. Please educate yourself before blowing off the idea. The option is not worth the small risk of using DEET.
I will continue to send out a reminder as we move into warmer weather. I also plan to post an update on my health progress from living with Lyme.
As the temperatures warm the chances of encountering ticks increase. I had a PA recently say we don’t have Lyme in Texas, what? Yes, Lyme or tick boring illnesses are in every state. Some states have a higher percentage of cases but dot fool yourself, tick-borne illnesses are in every state in the United States. There are now 30 strains of tick-borne illnesses and more are discovered each year. This year a more deadly tick-borne illness, Powassan Disease was discovered and it’s the most deadly. Please take notice and protect yourself and your children.
This post is a combination of photos, snippets from the previous posts, and new information. If you have questions visit ILADS website for the most accurate information on tick-borne illnesses. This association is for doctors who treat Lyme, educators of Lyme, and the medical community who are there to increase knowledge.
I am walking after four years spent in bed, how could anything be worse than Lyme Disease? The illnesses Lyme leaves behind are debilitating and worst. I’ve lost four years of my life, screaming in pain, narcotics, nine months of twice a day IV Antibiotic Infusion Treatments. I can not stress enough how dangerous Tick-Borne illnesses are, they can kill you and your children. If you already have a compromised immune system, your starting behind the curve. I’ve talked to many at WordPress with Chronic Lyme, many of them spent 10-15 years before diagnosis. Think of the pain and isolation of our fellow Bloggers went thru.
People have said we don’t have ticks, for one Lyme and Powassan Disease is transmitted by many sources other than ticks, mosquitos, sand flies, are just a few culprits. In the wild animals of all types of animals die, many pests visit the buffet. The critter who is carrying Lyme disease bites you and there is a short window for medical attention.
The flying pest target is blood, they have to eat. They don’t discriminate on where they go for lunch. The ticks who carry Tick-Borne illnesses are smaller than a grain of rice, try to find that while doing a tick check, you will not see them.
Before you get dressed, spray sunscreen with insect repellant with 20% DEET. Reply every hour if sweating or in heavily wooded areas. Wear white socks with your pant leg tucked in light-colored pants. Wear a white or light-colored shirt, a hat that is longer in back to cover your neck. Be vigilant with your kids, if playing outside, spray. Better safe than sorry.
Most important, do tick checks on you and the kids throughout the day. Take some tape and if you see a tick don’t touch it, pull it off with tape. While out hiking wear light colors, tuck pants in socks, wear a hat that covers the back of the neck. Lyme Dieses is not sexy.
Watch these extremely important videos and educate yourself. Know the early signs and a short antibiotic treatment may provide a cure. The bulls-eye rash talked about by doctors only happens 30% of the time.
The Lyme test doctors use only cover a few of the 30 strains of Lyme. I’ve had multiple tests over the past four years and not once did I show positive for Lyme.
Chronic Lyme disease causes other chronic illnesses in its wake and new illnesses can pop up at any time. I now suffer from Fibromyalgia, Dementia, Neuropathy, loss of balance, and other cognitive issues. My life is not back to normal and never will.
Chaos
State of Living Seven days of IV’s
IV Antibiotic Infusion Therapy
Sterile Living
Medical Waste
Port Inserted
Container for sharps
B12 Shots
Meds first three months
Port RemovedShaved HeadWigCrowded Bedside TableStaying organized Tracking computer My brain waves.
Over the past seven years I’ve seen: five primary care doctors, two neurologists, five OB-GYNs, one gastroenterologist, two urologists, one allergist, five dermatologists, five ER doctors, three functional medicine doctors, one ophthalmologist, one naturopath, four physical therapists, seven acupuncturists, and two craniosacral therapists—on a quest to find answers about my health.
I’m not a layperson. I wasn’t lost in the healthcare system. I know healthcare from the inside out. I have been a nurse for 17 years. I researched every doctor before scheduling an appointment. I prepared a list of questions and concerns for each doctor’s visit. Yet my outcome was misdiagnosis and dozens of prescription medications being thrown at symptoms.
Missing the root cause
If I’d been correctly diagnosed from the start, I could have avoided the following: Botox injections to my scalp and occipital nerve blocks to alleviate debilitating migraine pain and occipital neuralgia; an endoscopy; CT scans; MRIs; numerous ultrasounds; and countless lab tests. Not one doctor was able to determine the cause of my health problems. For starters, most weren’t looking for Lyme disease. Medications served as band-aids, and I was faced with the stark reality that the medical establishment I’d served for so long had failed me.
I hiked regularly in the Bay Area and had a dog when odd symptoms began to appear in 2013. Over the years, I would address one symptom, only to have another emerge months later. Sometimes I’d feel relatively okay for months at a time. My health improved somewhat after being treated for gut dysbiosis, worsening migraines, and interstitial cystitis. However, no one could pinpoint the root cause of my growing list of ailments. And I never felt fully well, like my old self.
In 2016, I saw a naturopath who tested me for Lyme disease as part of my new patient workup, using the standard serological ELISA and Western Blot lab tests. I read my results over and over. Negative. Negative. Negative. At the time, I didn’t know about the unreliability of the CDC’s two-tier testing protocol for Lyme disease. I was just told that Lyme had been ruled out. I’d tested negative, had never seen a tick, felt a bite, or had a bull’s-eye rash.
A Diagnosis
My health was in a downward spiral by the start of 2020. I still didn’t know what was causing my decline, I just knew I needed answers. A friend referred me to an integrative doctor who specializes in treating complex cases. It turns out, he’s a member of ILADS and has a lot of experience in recognizing and treating tick-borne illness.
As he looked over my lab results and read my list of chief complaints, he raised the possibility that Lyme disease could be at the root of my health problems. I couldn’t believe it! Had it been Lyme all along? My body was fighting something and perceived everything as a threat. Overactive mast cells translated into a myriad of symptoms ranging from histamine intolerance to anxiety and insomnia. He diagnosed me with mast cell activation syndrome, prescribed medications to stabilize my mast cells, and we agreed to test for Lyme disease via a specialized lab. My physical symptoms were beginning to make sense. I finally felt like I was headed in the right direction.
Health Inequity, Racial Disparities, & Implicit Bias
Once I was officially diagnosed with tick-borne disease, I joined a number of Lyme support groups. I was determined to find answers and connect with others battling the disease. As I explored each group, I noticed most members were white. I yearned to see representation in these groups. Why were so few people of color diagnosed with Lyme and other tick-borne infections?
As I’ve come to learn, there are many layers to that answer. A textbook bull’s-eye rash indicative of Lyme will present differently in people with dark skin. If the assessing doctor isn’t Lyme-knowledgeable, this cardinal sign may be missed. Latinxs are at high risk for contracting tick-borne infections due to occupational exposure. They comprise 44% of ground maintenance workers and 43% of farm workers. Because of health inequity, Black and Brown communities often lack access to healthcare.
Furthermore, access to Lyme-literate medical doctors (LLMDs) is problematic, as most are not in-network with health insurance plans. Thus, the cost of treatment falls squarely on the patient’s shoulders. Language barriers, fear of deportation, work schedules, and seasonal labor are roadblocks to seeking care early on as well. Lastly, a doctor’s bias, implicit or not, will directly impact if and when a diagnosis is made and how a patient’s complaints are treated. One study showed that doctors who harbor pro-white implicit biases aree more likely to prescribe pain medications to white patients than to Black patients.
CDC
Another barrier to diagnosis is the CDC’s rigid definition of Lyme disease. California, where I live, is considered “low-incidence” by the CDC. This means a patient in my state must meet a higher standard to be considered positive for Lyme, as compared to people in “high incidence” states.
The CDC also adheres to the Lyme treatment guidelines of the Infectious Diseases Society of America. According the IDSA, clearing Lyme disease only takes a few weeks of antibiotics. If symptoms persist beyond that, they call it “Post Treatment Lyme Disease Syndrome,” and advise against any further treatment. This also makes it easier for insurance companies to refuse to pay for Lyme medical care beyond the short course recommended by the IDSA.
Now four months into treatment with intravenous and oral antibiotics, I am beginning to see more and more glimpses of “the old me.” I hope to finish up sometime this year. I feel fortunate to have found a treating doctor to help me solve my health puzzle, along with caring and skillful nurses that never miss with IV placement.
I’m also grateful to have found an acupuncturist who has successfully treated Lyme patients for decades. She has helped my body detoxify and feel calmer, month after month. Everyone deserves to have holistic care, with integrative doctors and acupuncturists working collaboratively with a patient-centered approach. Sadly, this is not the case in our broken healthcare system.
Gabriela Wijegunawardena lives in the San Francisco Bay Area. This guest post is adapted from her blog Raising the Revolution.
Thank you for all the wonderful comments about this post each week. I appreciate you taking the time to write me the notes. When I hear about a product someone is using and I can use it, I’m glad they mentioned the product. I hope you find some products you can use in these posts.
I buy almost everything off of Amazon because they are often less expensive and as a Prime Member we get two-day free delivery. Also, if you use the Amazon Store Card you receive 5% back on all of your purchases. I’m all about saving money and free money!
Our fan-favorite collection of skin soothers is powered by a Centella Asiatica (Tiger Grass) complex to calm sensitive skin, reduce redness, and soothe irritation.
One small jar will last long after the expiration date. I realized mine was about two years old and had to purchase a new jar, the smallest size they had this time. Use this the minute you feel a pimple coming on and by day two it may be completely gone. It’s also great for covering up dark spots on your face. A tiny bit goes a long way!
Micellar technology, Gently cleanses and soothes, Removes makeup from face and eyes, Provides an instant feeling of freshness
Sensible H2O Facial Cleansing Wipes
I read Victoria Beckham used them, she has great skin so I had to try them. Surprisingly they are less expensive than many facial wipes on the market. I found them on Amazon and buy the two-pack. They are perfect for my sensitive skin. I don’t wear make-up these days so I only use these to clean my face with and a little toner. Available in the UK and many countries.
They smell is out of this world, no nasty smell, two pumps is all it takes and it dries fast. Your hands even smell good after since it’s made with essential oils. I also love the Lavender scent. I have purchased at Whole Foods in the past but now buy by the case off Amazon, it’s less expensive. Whole Foods charged over $4.00 a bottle the last time I checked.
We feed our dogs Natural Balance dog food and they love their snacks. We’ve tried every flavor and they haven’t snubbed their nose once. There are no fillers, no artificial flavors or colors, and no corn, wheat, or soy. We put them in Kong toys and they love it. Natural Balance is much better for them than the Kong brand treats and less expensive.
Leilani is an Indigenous CHamoru* and Kānaka Maoli woman, an activist, a life-long writer, and a survivor of sexual violence. On her second day of college, she was sexually assaulted by her dorm neighbor. The sexual violence continued in the form of an abusive relationship over the course of the next year.
“He was my neighbor. I couldn’t get away from him. No one would listen to me when I told them what was happening. I was horrified.”
Though she was able to leave the abusive relationship, the perpetrator stalked her for the next two years.
She began her journey of speaking out by reporting the abuse to the school. At the time, she was working in the community safety department on campus, so the person she was supposed to report the abuse to was her boss.
“He ignored a lot of my questions about the reporting process and made me feel like I was hysterical and crazy.”
After a first investigation into the case, the Title IX process took another two years.
“I lost my entire time at college to these procedures.”
Even though she provided witnesses and photos for evidence, campus administration repeatedly told her that they did not believe her.
“After two years of being told that I made this all up, it became difficult to continue to believe in myself. I began to feel like maybe it was all my fault.”
She found it healing to surround herself with a community of other Indigenous women who supported her and helped her contextualize what she was feeling within the history of sexual violence toward Indigenous women. Leilani says that she would not have been able to get through what happened without connecting with her identity as an Indigenous woman.
“Indigenous women face rates of sexual violence well above the national average, and you don’t hear many people talking about the missing and murdered Indigenous women epidemic….This community of women understood my experience so deeply and personally. ”
Activism has been another crucial part of Leilani’s healing process. For the last several years, she has worked on drafting laws and collaborated with congressional representatives about how best to support campus sexual assault survivors and prevent these crimes from happening on campuses. Leilani wants to ensure that others don’t have to go through what she did.
“I felt powerless for so long, and by fighting for others, I reclaim my power.”
Leilani has also found a lot of healing in connecting with support specialists on RAINN’s hotline—especially when she knows she has an urgent need and nowhere else to turn. Thank you,
Team RAINN💙As many students prepare to go back to college this fall—whether in person or online—let’s follow Leilani’s example and work to ensure that they can do so safely. RAINN has produced some tips on how students can return to campus safely. Please take a moment to share them with your networks on Instagram and Facebook today.DONATE TO SUPPORT SURVIVORS
Imagine, for a moment, living in a world where strep throat wasn’t treatable. Where getting a cut or a blister could be life-threatening, even for people in countries with well-developed health systems.
While this may seem far-fetched, that’s exactly what could happen if our antibiotics lose their ability to treat bacterial infections. For years, scientists have been warning usaboutthis scenario and telling us about the alarming rise in drug-resistant bacteria — but it doesn’t have to be our future.
Read on to learn 9 facts about antibiotics and how they were discovered, how bacteria learn to outmaneuver them, and how a bold idea (supported by The Audacious Project at TED) could help us address this problem.
So how did we get here?
1. We only have penicillin because of a scientist’s vacation and a policeman who grew roses
Penicillin, the first widely-used antibiotic, was discovered in 1928 and went on to revolutionize medicine. But we only have this drug — which treats strep throat, meningitis and more — thanks to a string of random events.
After his annual summer vacation, bacteriologist Alexander Fleming returned to his lab in London. When he was there, he realized that he had forgotten to place a petri dish in an incubator. As a result, an unusual mold was growing there. What’s more, the staph cells that he’d been studying and were clustered around it had actually died. Fleming called the mold “penicillin”, but then he struggled for more than a decade to isolate its active ingredient.
A group of biochemists at Oxford University — Howard Florey, Ernst Chain and Norman Heatley — picked up the charge. In 1940, they succeeded in purifying penicillin and tested it, first on mice and then on its first human subject: a policeman who’d contracted a life-threatening infection after being scratched by a rosebush in his garden.
At the same time, England was deep in the midst of World War II. According to the book The Mold in Dr. Florey’s Lab Coat, the group made a plan for what to do if Germany invaded — they rubbed penicillin spores into their lab coats so they could carry on their work should they have to flee.
That didn’t come to pass, but Florey and Heatley did have to solicit outside help to get penicillin mass-produced. They worked with both pharmaceutical companies and the US government to develop methods for growing penicillin at scale. By 1943, the US was supplying all the Allied forces with this miracle drug, which gave them a huge advantage in treating injuries.
2. Most of our existing antibiotics were found in the dirt — with the help of pilots and missionaries
Penicillin set off a golden age of antibiotic discovery, with scientists racing to identify substances with similar properties. At Rutgers University, agriculture student-turned-microbiologist Selman Waksman systematically tested an astonishing 10,000 soil samples over the course of his career. In 1943, he identified streptomycin, a broad-spectrum antibiotic effective against tuberculosis.
This work quickly got the attention of drug companies, who also set their eyes on searching soil. As public health journalist Maryn McKenna notes, Pfizer commissioned pilots, explorers and foreign correspondents to send back soil samples as they traveled; Eli Lilly, meanwhile, made a deal with the Christian and Missionary Alliance to have its members do the same. Bristol-Myers tapped its shareholders, asking them to mail in soil from wherever they went.
This tactic worked for decades, netting dozens of new antibiotics. But by the mid-1970s, researchers scouring soil samples found themselves discovering the same molecules over and over. Nothing new.
3. Discovery of new antibiotics has slowed, while bacteria are growing resistant to existing drugs
For the past 40 years, scientists have focused on methods like genomic sequencing to help identify new antibiotics. This process is slow and expensive — it costs roughly $1 billion per drug, says McKenna — and has yielded relatively little in the way of results.
At the same time, bacteria are learning to withstand our available drugs. They’re developing antibiotic resistance — sneaky strategies that prevent an antibiotic from damaging their cells. What’s more, bacteria appear to be getting more and more efficient at this. As McKenna explains in a TED Talk, vancomycin was first prescribed in 1972, and then vancomycin-resistant bacteria emerged in 1988. Imipenem came out in 1985, and resistance was noted in 1998. More recently, daptomycin came out in 2003, with resistance noticeable by 2004.
4. The very use of antibiotics increases the mutation rate of bacteria
Antibiotics are mutagens, which work by attacking a bacteria cell. If they don’t kill it outright, they trigger the cell to fight for survival. So the use of an antibiotic increases the probability of a bacteria cell mutating in a way that gains resistance.
Resistant cells are able to pass on new coding to their offspring with startling speed — bacteria birth a new generation every 20 minutes. Plus, cells are even able to hand off their resistance to other bacteria. As McKenna puts it in her TED Talk, “Bacteria can pass their DNA to each other like a traveler handing off a suitcase at an airport. Once we have encouraged that resistance into existence, there is no knowing where it will spread.”
Resistance can also accumulate. Some communities of cells now have resistance to multiple antibiotics, and these hard-to-kill bacteria are the “superbugs” that you’ve probably heard about.
5. Antibiotic resistance is a natural phenomenon, but overusing antibiotics makes the problem much worse
Given how swift bacteria are at building resistance, the best strategy for ensuring that antibiotics stay effective would be to use them sparingly and only when needed. But that isn’t what we’ve done.
In some countries, antibiotics are available without a prescription, and in Europe and North America, antibiotics are vastly overprescribed by physicians. Too many patients pressure practitioners for antibiotics, even for colds or viruses that can’t be cured by them. According to the US Center for Disease Control, 30 percent of antibiotic prescriptions written in the US — in doctors’ offices and hospitals — are unnecessary.
6. Antibiotic use in livestock and antibacterial soaps are also driving resistance
In the US, 70 percent of all antibiotics sold are used on farms to fight off infections in livestock and enhance their growth. Antibiotics are also used in the farming of fish and shrimp, as well as in the growing of fruits like apples, pears and citrus even though they’re not always necessary.
Meanwhile, consumers’ use of antibacterial soaps are on the rise. Then, with the COVID-19 pandemic, many people are using hand sanitizer gels and disinfecting wipes much more frequently. It’s the right thing to do while the virus is a threat — but in the long run, it could further stoke resistance.
7. The number of people dying from antibiotic-resistant diseases keep rising
According to a 2019 report from the World Health Organization, at least 700,000 people are already dying of drug-resistant diseases each year. That number could rise to 10 million annually by 2050, making antibiotic resistant infections more deadly than cancer. We could soon be living in a very different world, one where the medical advances of the last century are wiped away.
8. But there is good news: Artificial intelligence has helped identify the first new broad-spectrum antibiotic in decades
This story promised hope, and that’s where the work of the Collins Lab at MITcomes in. Led by synthetic biologist Jim Collins, the lab has the goal to speed up the process of discovering new antibiotics and replenish our antibiotic arsenal. They’re doing this by harnessing the power of machine learning to screen unprecedented numbers of molecules for antibiotic properties.
In a 2020 study, Collins’ team announced that they have identified a new, highly-potent antibiotic: halicin.Named for HAL 9000, the sentient computer in 2001: A Space Odyssey, it seems to have real superpowers. Halicin rapidly kills E. coli, M. tuberculosis and more, and it’s also effective against the antibiotic-resistant bacteria that cause sepsis and pneumonia.
Equally important, halicin doesn’t appear to trigger mutations like other antibiotics do — while E. coli can develop resistance to other antibiotics in a single day, it wasn’t able to develop resistance to halicin even after 30 days of exposure. While scientists have known about halicin for a while — it was tested as a treatment for diabetes years ago — no one suspected it had antibiotic properties. “It doesn’t look like the antibiotics we know, so it would have been all but impossible for humans to recognize it as an antibiotic,” says Collins.
Thanks to the support of The Audacious Project, the funding initiative housed at TED to catalyze ambitious ideas into action, the Collins Lab is looking to add to our antibiotic toolbox. Their mission is to identify seven new classes of antibiotics to tackle seven of the world’s deadliest bacterial pathogens over the next seven years.
The lab’s work begins by analyzing the antibacterial activity of 100,000 known molecules. From there, they’ll train a machine-learning model to predict — based on their chemical structure — whether the new molecules could kill bacteria. Somewhere in this process, they should find antibiotics perfectly suited to fight ultra-deadly bugs. Researchers can also use what the model learns about antibacterial properties to design entirely new molecules that could be synthesized and tested.
9. Even better: This method might also have an impact on COVID-19
As Collins shared in his TED talk, he and his team are training an AI platform to search for new antivirals that could treat COVID-19. At the same time, they’re looking to modify the BCG vaccine — currently used to prevent tuberculosis — to include COVID-19 antigens. Finally, they’re working to create a face mask that could continually test its wearer for COVID-19 as they breathe (wow!). They’ll do this by freeze-drying RNA sensors onto cloth.
One last thing: Combating antibiotic resistance isn’t just the work of people like the Collins Lab team. We can each do our part
Next time you’re sick, double-check with your doctor to make sure an antibiotic is really necessary. If it is, be sure to follow the prescription instructions so that you kill the bacteria rather than drive mutation. In your everyday life, you can look for antibiotic-free meat and buy plain soaps rather than antibacterial ones — they’re just as effective on virus particles.
Yes, it’s hard to think about facing another large-scale global health crisis in our lifetimes — but we have a chance to heed the warning this time.
ABOUT THE AUTHOR
Kate Torgovnick May is a journalist and writer based in Los Angeles. A former storyteller at TED, she has worked with the ambitious thinkers of the TED Prize and Audacious Project, helping them share their stories in video and text. She’s also the author of the narrative nonfiction book, CHEER!: Inside the Secret World of College Cheerleaders, and has written for the television series NCIS and Hellcats. Read more about her work at KateTorgovnickMay.com.
I’m so glad you joined me this weekend, I hope you have a great weekend. Be Safe. This week I share one of my favorite Rolling Stones tunes and provide two live videos and you will get a real kick out of. I love the fashion of the time and the differences in each video. :)
Melinda
Welcome back to Weekend Music Share; the place where everyone can share their favorite music.
Feel free to use the ‘Weekend Music Share‘ banner in your post, and don’t forget to use the hashtag #WeekendMusicShare on social media so other participants can find your post.
P2 powers internal collaboration at WordPress.com — and now it’s free for everyone. As more collaboration is happening remotely and online — work yes, but increasingly also school and personal relationships — we’re all looking for better ways to work together online. Normally, teachers hand out homework to students in person, and project leaders gather […]